Protected: Turning lived experience into innovation: How Tamara Tortosa is building Qalyup
A resident doctor reviews a patient late in the day. The presence of an infection is uncertain. The guidelines are long and complex, and time is limited. The consultant wants a decision. The patient is expecting treatment.
Does the doctor prescribe antibiotics or not?
This is the reality of antimicrobial prescribing in hospitals. Decisions are often made under pressure, shaped not only by clinical evidence but by time constraints, hierarchy and patient expectations. These decisions matter. Every unnecessary or inappropriate prescription contributes, in small but cumulative ways, to a much larger global challenge: antimicrobial resistance (AMR).
AMR occurs when microbes such as bacteria, viruses, fungi and parasites no longer respond to the drugs used to treat them. It has been described as a “silent pandemic” because it builds gradually – in infections that take longer to treat, in extended hospital stays and in the slow narrowing of effective treatment options.
The scale of the challenge is stark. Global estimates suggest that AMR was associated with 4.95 million deaths in 2019.
Research led by Dr William Waldock, Clinical Research Fellow at our NIHR Northwest London Patient Safety Research Collaboration and supported by the Fleming Initiative and published in Nature npj responds to this wider challenge by exploring how antimicrobial resistance can be better measured across healthcare systems and addressed in clinical decision-making.
AMR is not just a scientific challenge; it is also behavioural and systemic. The knowledge needed to prescribe antibiotics correctly already exists in clinical guidance, alongside diagnostic information. Yet across hospitals and community care settings, this guidance can be difficult to use, inconsistently applied or overridden altogether.
In Dr Waldock’s two recent studies, the researchers set out to address this challenge from two complementary angles: how antimicrobial resistance is measured within healthcare systems and how clinicians can be better supported to make prescribing decisions in real time.
If AMR is such a significant global threat, why is it so difficult to control? Part of the answer lies in how it is measured.
Traditionally, AMR has been tracked through surveillance data – monitoring which bacteria are resistant to which drugs and where those patterns are emerging. While this provides an important picture, it does not always capture how resistance is experienced within healthcare institutions.
In the first study – Development of the antimicrobial resistance burden score through a modified eDelphi – the researchers highlight this gap and propose a new approach.
The study shows that relying on isolated indicators can be misleading. A hospital with high antibiotic use may still be practising strong stewardship, while another with lower reported resistance rates may reflect limited diagnostic capacity or incomplete reporting.
The AMR Burden Score brings these different measures together into one structured view, combining resistance patterns, prescribing practices and clinical outcomes. This allows healthcare organisations to better understand their AMR burden and assess whether interventions are making a meaningful difference over time.
In doing so, it provides a more integrated and interpretable picture of AMR within healthcare systems, allowing patterns to be tracked over time and the impact of interventions to be more clearly assessed.
If measuring AMR is one part of the challenge, the other lies in how prescribing decisions are made.
Antibiotic prescribing is rarely straightforward. Clinicians often need to make decisions quickly, sometimes with incomplete information, balancing the risks of under-treating infection against those of unnecessary antibiotic use. While guidelines exist to support these decisions, they are not always easy to apply in busy clinical environments.
The research highlights how this complexity plays out in everyday care, where time pressure, workflow design and differences in clinical judgement all influence how guidance is applied.
As Dr Waldock explains:
“In-hospital antimicrobial prescribing is frequently driven by the urgency of a deteriorating patient. While diagnostics are vital, clinical reality often demands pre-emptive intervention before full data is available. Junior doctors may occasionally have senior guidance, but more often, they must navigate these high-stakes initial prescriptions alone. In such moments, objective and accessible resources to guide the first response are invaluable.”
In this context, prescribing decisions are not made in isolation. They are shaped by interactions between clinicians, patient expectations and wider system pressures. This can create situations where decisions that seem appropriate for one patient in the moment may conflict with longer-term public health interests.
As Dr Waldock puts it:
“This reflects what economists call the ‘tragedy of the commons’ – where individual decisions, whether driven by clinical caution, patient expectation or organisational pressure, can work against the long-term interests of the wider population.”
This helps explain why improving antimicrobial use is not simply a matter of producing better guidance. The challenge is not only what clinicians should do but also how they are supported to make decisions in complex clinical environments.
It is this gap between knowledge and its application that the second study seeks to address.
If AMR is shaped by everyday prescribing decisions, the next challenge is how those decisions can be better supported.
In the second study – Enhancing quality of antimicrobial prescribing through ‘Ask Eolas’ (language model): a user-testing and simulation evaluation – the researchers explored how AI can support prescribing decisions in clinical settings.
Ask Eolas is an AI-supported clinical decision tool designed to help clinicians access the right antimicrobial guidance more quickly and accurately. The tool retrieves and summarises reliable clinical guidance while providing clear links back to source material, allowing clinicians to verify its recommendations.
On the value of Ask Eolas in clinical settings, Dr Waldock notes:
“Ask Eolas appears to make the prescribing process much safer and more reliable. Unlike previous tools that could feel like a ‘black box’, this technology is transparent about why it is making a suggestion. This gives clinicians more peace of mind and makes their daily workflow feel much smoother.”
In a structured simulation study, Ask Eolas outperformed both traditional PDF guidelines and existing digital tools. Participants using the system achieved fully accurate prescribing decisions across the study scenarios.
Clinicians also reported higher confidence and lower cognitive workload when using the tool, describing it as clearer and easier to use than traditional guidance formats.
This highlights that improving antimicrobial use is not only about providing the right information, but about presenting it in a way that can be used effectively under pressure.
While these findings are based on a controlled simulation, they provide early evidence that carefully designed AI tools could support safer and more consistent prescribing in clinical settings.

Together, these two studies outline a more connected approach to antimicrobial stewardship, where better data and better decision-making reinforce one another.
The AMR Burden Score provides a more complete view of how AMR is developing within healthcare systems, while Ask Eolas supports clinicians to make more accurate, evidence-based prescribing decisions in real time.
This reflects a wider transformation in healthcare. Rather than relying solely on static guidance and retrospective review, there is growing interest in more responsive systems that can support clinical decisions as they are made.
Looking ahead, Dr Waldock points to a move towards a more “agentic” hospital:
“The agentic hospital is a shift from doctors using tools to doctors leading a team of ‘agents’ in the delivery of healthcare. Instead of a computer just holding your medical records, it’s now an ‘agent’ that supports your care: spotting risks before they happen, coordinating your tests instantly and handling the paperwork so your doctor can spend their time focusing entirely on you.”
There is still more to do. Both studies highlight the need for further validation, real-world testing and continued collaboration across healthcare systems. They also demonstrate what is possible when research is grounded in real clinical challenges and designed with end users in mind – central to the Fleming Initiative’s work in harnessing technology for real-world impact.
AMR may be shaped by decisions made every day. Strengthening how those decisions are supported in clinical settings will be central to any meaningful response.
This blog was co-authored by Helix Centre designers Sophie Horrocks and Tori Simpson.
From care pathways to medical products, healthcare can (and must) be designed to minimise waste, reduce emissions, and protect planetary health. This is not a distant vision, but an urgent necessity. As the world’s leading designers gather for the World Design Congress themed Design for Planet, here at the Helix Centre, we are exploring what it will take to make this ambition a reality, and the role human-centred design in healthcare can play in achieving it.
The connection between climate change and human health is increasingly clear. More frequent and severe heatwaves, floods, droughts, and storms directly harm health through injuries, heat stress, and other acute impacts. These events also indirectly affect communities by altering the spread of infectious diseases, driving food and water insecurity, damaging infrastructure, and deepening existing inequities. Together, they contribute to excess deaths and worsening physical and mental health outcomes (Haines et al., 2006; The Lancet, 2024).
Healthcare is also part of the problem. Globally, health systems produce around 5% of national CO₂ emissions in OECD countries (Pichler et al., 2019). In the UK, the sector accounts for 4–5% of total emissions, with the NHS in England responsible for about 40% of the public sector’s footprint (British Medical Association, 2024). At the same time, the climate crisis threatens the resilience of healthcare itself, with extreme weather disrupting services and rising health burdens straining already stretched systems.
These twin pressures highlight the urgent need for sustainable healthcare. By this, we mean the provision of health services in a way that meets the needs of today’s populations without damaging the health (or the ability to meet the healthcare needs) of people separated from us by time, geography, or socioeconomic status.
The challenge is significant, but it also highlights healthcare’s huge potential to drive change. Designing sustainable healthcare involves navigating trade-offs, such as balancing sterility requirements with reducing the footprint of medical equipment, while also seizing “win-wins” that benefit health, the environment, and even social and economic wellbeing.
At the Helix Centre (and Imperial College London’s Institute of Global Health Innovation more broadly) we’re exploring this challenge through six “wicked problems” at the crossroads of healthcare and sustainability. We have mapped these onto a matrix with the following axes, and for each, we share how we define the issue, present a case study of inspiring work in the field, and highlight sessions we plan to attend at the World Design Congress to deepen our understanding.
Through this article, we aim to open a conversation on how designers and other practitioners working in healthcare delivery (ourselves included) can integrate sustainability challenges into the heart of their work. If these themes resonate with you, we’d love to hear your ideas and examples and explore together how we can create healthcare systems that protect both people and the planet – get in touch with us at climate@helixcentre.com.

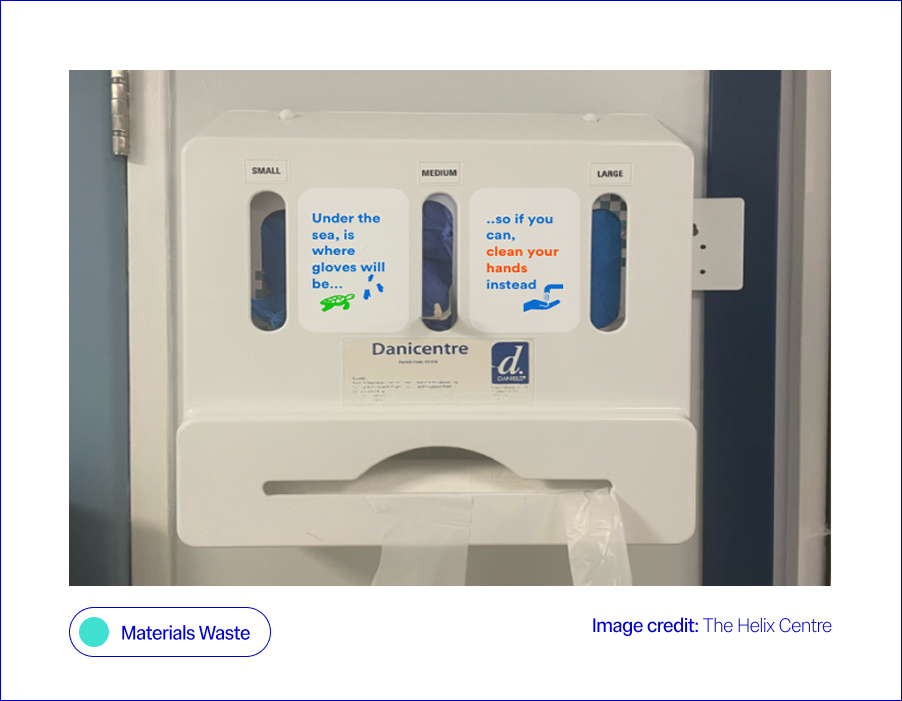
Every year, NHS England providers produce 156,000 tonnes of clinical waste. Tackling this could unlock major wins for both the environment and patient care. However, the answer isn’t simply reusing equipment. In healthcare, there is a complex trade-off between maintaining sterility requirements and limiting the environmental impact of medical equipment, particularly given that many essential items such as syringes and personal protective equipment (PPE) are single-use (Nicolet et al., 2022). Sterilising these single-use items for reuse can often be as carbon-intensive as replacing them after each use.
At Helix, we worked with a large NHS provider to test a behavioural “nudge” (a small design change that makes the sustainable choice easier without restricting options), aimed at improving hand hygiene practices and reducing the over-reliance on gloves. On hospital wards, glove use had become the default during the pandemic, often replacing standard hand hygiene practices like washing hands or using alcohol gel. To help staff return to safer, less wasteful habits, we co-designed a sticker for glove dispenser boxes, reminding staff when gloves were really needed. This small prompt (our “green nudge”) led to an 11% increase in hand hygiene compliance, meaning staff cleaned their hands more often at the right times, usually by washing with soap and water or using alcohol gel, in line with official guidelines (Blair et al., 2024). Outside of Imperial, the DesignHOPES team has worked with NHS staff to co-design a reusable theatre cap, designed to replace the current single-use ones. This intervention not only reduces waste but has also allowed for the personalisation of clinicians’ theatre caps, creating further wins for patient safety and staff identification. The Design for Life programme outlines an agenda and six fundamental challenges for our healthcare system in developing and embedding a circular system for medtech products.
Waste not, want not: from waste to wonder – a conversation between Sophie Thomas, Paula Chin, Adam Fairweather, Jo Barnard and Yaseed Chaumoo

What is the issue?
Care pathways are major contributors to the healthcare system’s carbon footprint. Fewer hospital visits, simpler procedures, and reduced prescribing could deliver large savings (NHS England, 2021). In summary, implementing quality improvement across care pathways with sustainability in mind can be a win-win in terms of environmental impact and patient outcomes (Health Foundation, 2025). Many trusts within the NHS are already assessing services against the Centre for Sustainable Healthcare’s all-encompassing definition of sustainability, which considers environmental, social and financial impacts as the foundational pillars in achieving sustainable services (NHS England, 2025). Alongside care pathways, food and transport services are listed as focus areas for the NHS’s green transition, cited as services that, if delivered more sustainably, could have a high impact on the NHS’s carbon footprint, with the two mentioned services comprising 20% of the health service’s total emissions (World Health Organisation, 2025).
Within Imperial, Matthew Harris explores opportunities for bidirectional learning between the NHS and low-income countries, including the implementation of various “frugal innovations” that use fewer resources to deliver healthcare, without compromising patient safety or clinical outcomes (Brown et al., 2023). Further afield, the GIRFT programme at Exeter University is developing a toolkit to map current carbon emissions and predict their impact on sustainability, financial aspects or care, patient outcomes, and equity of access. Within the NHS, the world’s first zero-emissions ambulance is being trialled in the West Midlands, setting an example for how other trusts can roll out more sustainable transport fleets, with the potential for dramatic carbon savings, given the NHS fleet is the second largest in the country (NHS England, 2023).
From Lab to Launch: How design accelerates Global Impact – an unconference with Paul Rodgers, Pete Broadbent, Suraj Vadgama, and Edward Hobson
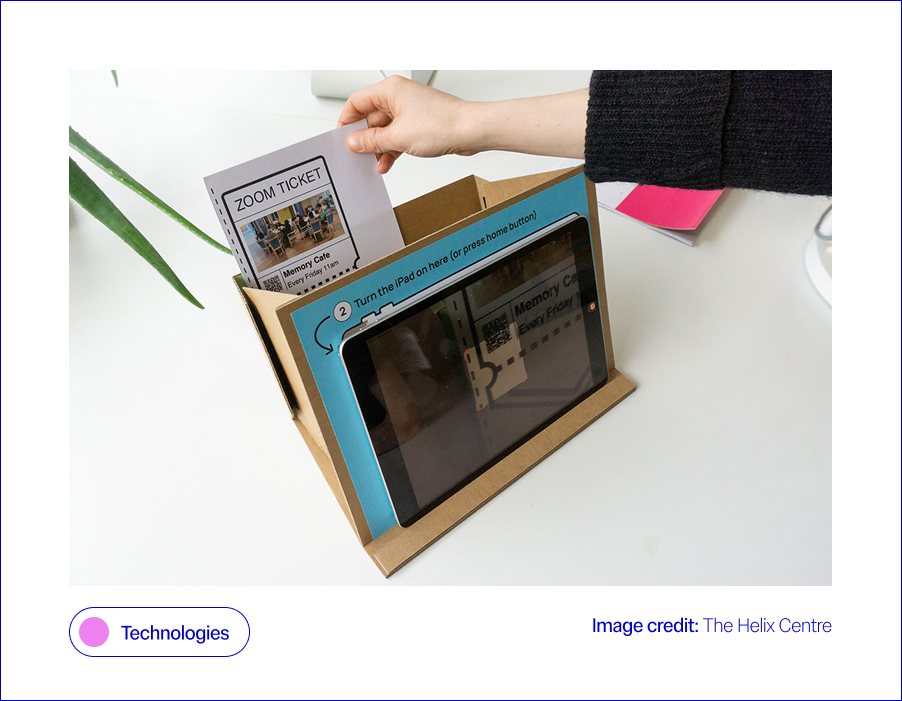
Technology, such as digital tools and remote monitoring to support care, is central to the NHS’s plan to cut emissions. Reduced transport costs, greater efficiency, and a focus on digital preventative care are all given as examples of how better use of technology could fast-track the NHS’s green transition (HSJ Information Ltd., 2025). However, with the intention to use AI systems to support many of these technologies discussed in the NHS’s recently released 10-year plan, it is important to consider the environmental impact of these technologies when implementing them (NHS England, 2025). It is estimated that globally, the data centres that power the technologies in question accounted for around 1.5% of global electricity consumption in 2024, with this consumption projected to grow by 15% per year (International Energy Agency, 2024). Similarly, a single data centre on average uses 300,000 gallons of water a day for cooling, enough electricity to power 100,000 homes (Ziegler, 2024). Finally, the move towards a more technologically enabled NHS also comes with a risk of digital exclusion for vulnerable parts of the population, which must be carefully considered within the transition (Health Innovation Network, 2023).
Previously, Helix collaborated with the London Office of Technology and Innovation (LOTI) to create a prototype system to support people with little experience of technology to participate in online meetings, mitigating the risk of digital exclusion as the healthcare system transitioned more to online engagement, following COVID-19, a decision that had a knock-on positive effect on carbon emissions (Rothwell et al., 2023). Within IGHI, Aws Almukhtar, supervised by Gaby Judah and Daniel Leff, is embarking on a project that will demonstrate surgical simulation as a novel research tool for testing and refining behavioural interventions designed to decrease carbon emissions from operating theatres. By testing interventions in simulated operating theatres, researchers can identify and refine the most impactful new approaches that improve sustainability and cut waste while maintaining quality before they ever reach a patient. Importantly, surgical simulation makes it possible to explore interventions, such as eco-labelling surgical instruments, that could not be tested feasibly in live operating theatres without prior supporting data.
Communities, AI, and Collective Impact – a panel discussion between Sevra Davis, Michael Bennett, Suma Balaram Schippers, Anne Asensio, Bharat Kapoor, Dr Ramit Debnath, Michele Morris, Jayden Ali, Mattie Yeta, and Dr Geke van Dijk
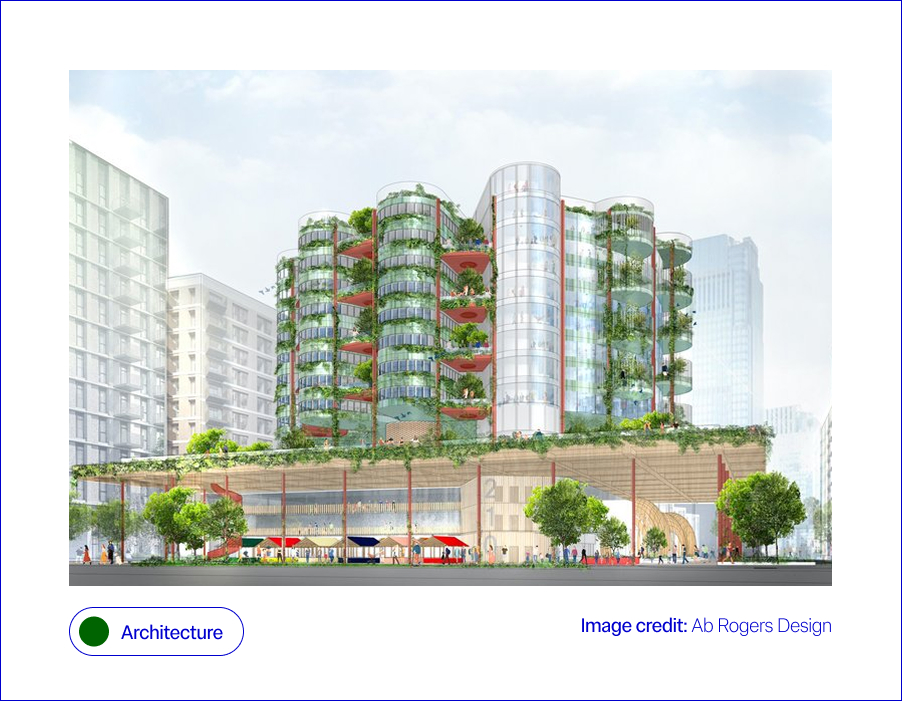
Hospitals are among the most carbon- and energy-intensive buildings, with 24/7 operations, complex equipment, and high heating and cooling demands. A 2024 systematic review highlights that hospitals contribute disproportionately to health sector emissions, with key drivers including energy use in buildings, embodied carbon in construction (the emissions tied to materials and construction), and waste streams (Public Health, 2024). Smarter building design and retrofits offer a clear path to reducing this impact. Alongside materials, “invisible” systems like ventilation or plumbing also affect sustainability performance and patient wellbeing. Climate change exacerbates these challenges, demanding that
hospital architecture becomes not only resilient to extreme weather, for example, floods and heatwaves, but also adaptive to future innovations. This means buildings must embrace digitally enabled architecture, where the physical fabric supports integration of new health technologies, automation, and data-driven energy systems (Design Council, 2021). In the context of architecture, sustainability is multi-layered, spanning bricks, wires, and human experience.
Responses span both future visions and practical action. Ab Rogers Design’s Living Systems reimagines hospitals as therapeutic spaces that integrate light, nature, and flexible layouts (RIBA, 2021). At a system level, the NHS Net Zero Building Standard (2023) is shifting net zero from exception to expectation. A powerful real-world example comes from Milton Keynes University Hospital, which re-roofed estate buildings and installed 2,586 solar panels. In 2021, these generated 853 MWh of electricity (around 8% of the hospital’s demand), cutting emissions, saving more than £225,000 annually, and improving patient comfort. The Trust plans to expand to 3,400+ panels, covering 15% of its needs (NHS England, 2021). Improving building resilience is also key: Loma Linda University’s hospital in California was designed to withstand seismic shocks, while UK trusts are retrofitting with double glazing and smart systems to reduce energy demand (Arup, 2023; BBC, 2023). Architectural consultancies like Buro Happold emphasise the need for adaptable hospitals that can withstand climate uncertainty while supporting patient wellbeing. Together, these examples show sustainability in healthcare estates is no longer aspirational; it is becoming standard practice for safer, greener patient care.
Design for Planet In Action: Fabrication, Futures, and Frontlines. Featuring: Samson Sahmland-Bowling, Peter Gitau, Alba Suárez Zapico, Charles Cambianica, Bethany Koby, Shajay Bhooshan
Building for the Future with Zoe Balmforth, Cameron Frayling, Hélène Chartier, Michael Pawlyn, Joanna Rowelle, Vanessa Miler-Fels
NHS England’s Greener NHS strategy identifies “models of care” as a priority, recognising that moving services from hospitals into communities can significantly reduce emissions while improving quality of and access to care (NHS Long Term Plan, 2019). This has been further emphasised by the recently released NHS ten-year plan, which sets out a vision for a “Neighbourhood Health Service”, which shifts care into local communities, to “reintegrate healthcare into the social fabric of places” (Department of Health and Social Care et al., 2025). Hospitals are resource-intensive, whereas community-based services allow greener, more localised alternatives through hub-and-spoke systems and preventative care.
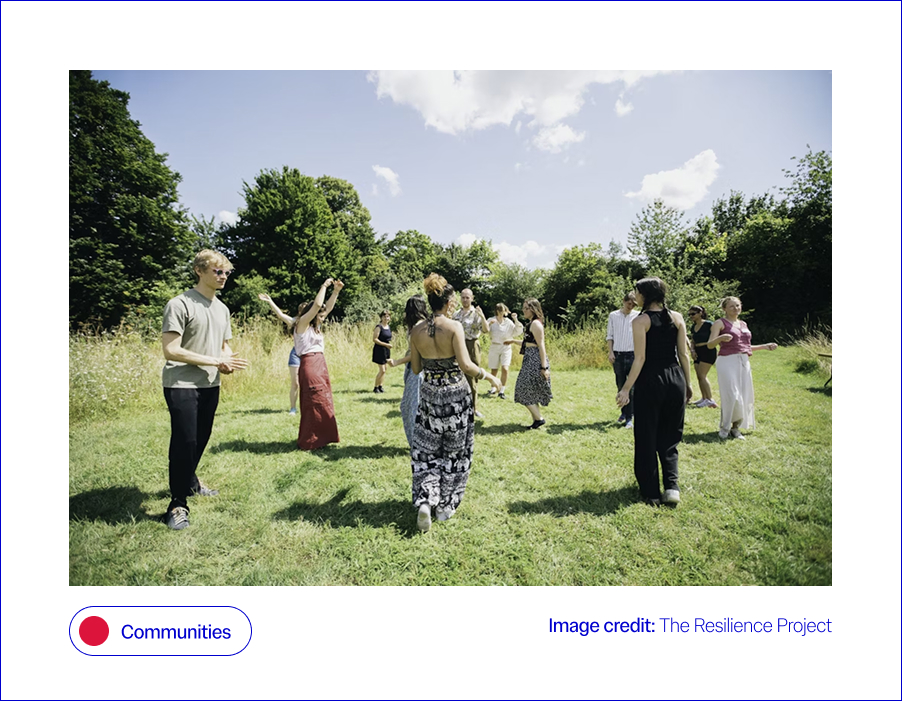
This shift is also vital for addressing the intertwined challenges of mental health and resilience in the face of climate change. Community-rooted care can provide both clinical and psychosocial support, enabling individuals and communities to adapt to climate-related stresses while easing pressure on hospitals. Community-based approaches, from preventative interventions to green social prescribing, demonstrate how models of care can reduce emissions while strengthening people’s physical and mental wellbeing (NHS England, 2021). Finally, any discussion of the built environment would be incomplete without noting the positive effects that access to nature and green space can have on health, mental wellbeing, and social connection, a powerful win-win where greener care spaces enhance both patient outcomes and climate resilience (Loveard, 2025). Ultimately, the challenge is not only to cut carbon but to reimagine care systems that also foster resilience, equity, and sustainability.
Innovative responses are emerging across different contexts. Within Imperial’s Institute of Global Health Innovation, the Climate Cares Centre is working with young people in the Philippines, Australia and the Caribbean to understand psychological responses to the climate crisis and co-design supportive interventions (Rising Faster than the Sea Levels). Climate Cares is also working to align climate change education and mental health support in schools and universities to support resilience building (the Compass Project). Climate Cares also works to connect and amplify existing initiatives around the world, such as ECO-MAMA, in Rwanda, which empowers women to safeguard mental health during climate stressors through an AI chatbot, and The Resilience Project in the UK, Europe and East Africa, which strengthens wellbeing through emotional regulation skills and social connection.
These programmes illustrate how initiatives can build resilience while broadening the ways in which care and wellbeing support are delivered. Building on this, research led by Matthew Harris has championed the role of community health worker models, drawing on international experience to strengthen local health delivery (Imperial College London, 2021). At the system level, the NHS has also expanded green social prescribing pilots, embedding nature-based activities into care pathways to support wellbeing and healthcare sustainability (NHS England, 2021). Together, these efforts sit within the broader framework of the NHS 10-Year Plan, which sets out a national roadmap for embedding greener, more personalised, and more resilient systems of care (NHS Long Term Plan, 2019).
Communities, AI, and Collective Impact featuring: Dr Geke van Dijk, Jayden Ali, Michael Bennett, Michèle Morris, Sevra Davis, Suma Balaram Schippers, Anne Asensio, Bharat Kapoor, Mattie Yeta, Dr Ramit Debnath

Sustainable healthcare requires action at every level, from national policy frameworks to the day-to-day choices of staff and patients. The climate crisis can feel like an added pressure for already stretched health systems, but there are clear “win–wins” to be found; just as insulating homes can cut energy bills and improve health whilst reducing emissions, similar opportunities exist in healthcare when policy and practice align. Top-down change is essential for embedding sustainability into governance, investment, and regulation, setting the conditions for lasting change. Simultaneously, bottom-up engagement is equally vital: sustainability can feel overwhelming or abstract for those working on the front line, so it matters how staff and communities understand and shape what is achievable in practice. Embedding resilience, therefore, requires not only policy and infrastructure but also a workforce that is equipped, supported, and motivated to act. Without this support, the resilience of the health workforce itself is at risk, with overwhelm and burnout threatening the very capacity needed to deliver sustainable care (Lawrence et al., 2024).
Behaviour change is a critical link between these levels; while many people recycle diligently at home, they may not apply the same habits at work or in public spaces such as hospitals. This underscores the importance of cultural as well as technical shifts, and the need to prioritise collective action, rather than an overemphasis on individual responsibility (Lawrance et al., 2022; van den Berg, 2015). Ultimately, progress depends on aligning ambitious policy with everyday behaviour change, supported by training and upskilling that empowers people at every level of the system (Michie et al., Behaviour Change Wheel).
Change is being driven from both the top down and the bottom up. At the policy level, the Health and Care Act 2022 made the NHS the first health system globally to embed statutory net zero and environmental duties into law, requiring NHS England, trusts, and integrated care boards to factor sustainability into their decisions (NHS England, 2022). This commitment is reinforced by the wider NHS Net Zero plan and efficiency-focused programmes such as Getting It Right First Time (GIRFT), which cut waste and emissions while improving care (GIRFT, 2024). At the organisational level, Green Plans provide a framework for trusts to set out three-year roadmaps towards more sustainable estates and services (NHS England, 2021).
Alongside this, bottom-up change is supported through training and workforce development: for example, the Climate Cares Centre at IGHI co-developed an Apolitical course, equipping policymakers with the knowledge and skills to address climate change and mental health simultaneously. Behavioural interventions are also crucial, helping staff to embed sustainable habits in clinical and operational settings; bridging the gap between what people already practise at home, like recycling, and what feels achievable in a healthcare context. To accelerate progress, policy must scale up these “win–wins” that make sustainable choices easier, so patients, staff, and organisations alike can help drive a greener future, through both everyday decisions and long-term strategies.
Designing the Economy We Need: Missions, Doughnuts, and Radical Collaboration with Mariana Mazzucato, Kate Raworth, Danny Sriskandarajah
The climate emergency is reshaping how we think about the way we provide healthcare. But this is also a design opportunity: to build systems that are not only safer and more effective, but also sustainable, resilient, and equitable. At Helix, we see our role as creating the conditions for this transformation: using human-centred design to tackle the toughest challenges at the crossroads of health and sustainability. The World Design Congress is a chance to learn, to share, and to build alliances with others who are equally committed to designing for the planet. Our contribution is to bring healthcare into this conversation, surfacing challenges, testing solutions, and creating space for collaboration. Beyond the Congress, we hope to serve as a bridge between designers and healthcare systems, so that bold ideas can become practical realities. By recognising these trade-offs and scaling the win–wins, we can design healthcare that is safer, greener, and more equitable, for both people and the planet.
With enormous thanks to Aws Almukhtar, Daniella Watson, Jessica Newberry Le Vay, Leila Shepherd, Matt Harrison, and Natalia Kurek, who have helped us shape our thinking in this space.
Arup (2023) Loma Linda University Health: Dennis and Carol Troesh Medical Campus. Available at: https://www.arup.com/projects/loma-linda-university-health-dennis-and-carol-troesh-medical-campus.
BBC News (2023) Milton Keynes Hospital installs solar panels to cut emissions. Available at: https://www.bbc.co.uk/news/articles/cz4dyj70dyvo.
Blair, C-J., McCrudden, C., Brazier, A., Huf, S., Gregory, A., O’Driscoll, F., Galletly, T., Leon-Villapalos, C., Brown, H., Clay, K., Maxwell, S., Anakwe, R. and Grailey, K. (2024) ‘A helping hand: Applying behavioural science and co-design methodology to improve hand hygiene compliance in the hospital setting’, PLOS ONE, 19(12), e0310768. doi:10.1371/journal.pone.0310768.
British Medical Association (2024) More support needed to help the NHS reach net zero. British Medical Association. Updated 28 June 2024. Available at: https://www.bma.org.uk/what-we-do/population-health/protecting-people-from-threats-to-health/more-support-needed-to-help-the-nhs-reach-net-zero
Brown, C., Bhatti, Y. and Harris, M. (2023) ‘Environmental sustainability in healthcare systems: role of frugal innovation’, BMJ, 383(8401), Article e076381. doi:10.1136/bmj-2023-076381.
Department of Health and Social Care, Prime Minister’s Office, 10 Downing Street, The Rt Hon Sir Keir Starmer KCB KC MP and The Rt Hon Wes Streeting MP (2025) Fit for the Future: 10 Year Health Plan for England. First published 3 July; updated 30 July 2025. Available at: https://www.england.nhs.uk/long-term-plan/
Design Council (2021) The Future of Health and Healthcare Design. London: Design Council. Available at: https://www.designcouncil.org.uk/fileadmin/uploads/dc/Documents/future-health-full_1.pdf.
GIRFT (2024) Getting It Right First Time: Net Zero and Sustainability. Available at: https://gettingitrightfirsttime.co.uk/cross_cutting_theme/net-zero-sustainability
Haines, A., Kovats, R.S., Campbell-Lendrum, D. and Corvalán, C. (2006) ‘Climate change and human health: Impacts, vulnerability and public health’, Public Health, 120(7), pp. 585–596. doi:10.1016/j.puhe.2006.01.002.
Health Foundation (2025) Why environmental sustainability must be at the heart of reform if the 10-year health plan is to help the NHS reap the benefits for patients, the health system and … [Blog]. Available at: https://www.health.org.uk/features-and-opinion/blogs/why-environmental-sustainability-must-be-part-of-the-10-year-health-plan
Health Innovation Network (2023) Bridging the Digital Divide in NHS Transformation: Ensuring Inclusivity and Equity [Blog]. Published 18 December 2023. Available at: https://healthinnovationnetwork.com/insight/bridging-the-digital-divide-in-nhs-transformation-ensuring-inclusivity-and-equity/
HSJ Information Ltd. (2025) Moving Towards Net Zero through Digital, HSJ Digital Awards [webpage]. Available at: https://digitalawards.hsj.co.uk/award-category/moving-towards-net-zero-through-digital
Imperial College London (2021) From Brazil to Westminster: Learning from a community health worker model. Available at: https://spiral.imperial.ac.uk/entities/publication/256305ad-73a4-4e7e-afa2-3c6af23369d2.
International Energy Agency (2025) Energy demand from AI. Paris: International Energy Agency. Available at: https://www.iea.org/reports/energy-and-ai/energy-demand-from-ai
Lawrence, W., et al. (2024) ‘Sustainable health systems and workforce resilience’, BMJ, 387, e081284. doi:10.1136/bmj-2024-081284.
Lawrance, E.L., Thompson, R., Newberry Le Vay, J., Page, L. and Jennings, N. (2022) ‘The Impact of Climate Change on Mental Health and Emotional Wellbeing: A Narrative Review of Current Evidence, and Its Implications’, International Review of Psychiatry, 34(5), pp. 443–498. doi:10.1080/09540261.2022.2128725.
Loveard, D. (2025) ‘Nature for Health: Making Green Space Work in Healthcare’, NHS Forest Blog, 23 June. Available at: https://nhsforest.org/blog/nature-for-health-resource-hub/
Michie, S., van Stralen, M.M. and West, R. (2011) ‘The Behaviour Change Wheel: A new method for characterising and designing behaviour change interventions’, Implementation Science, 6(42). doi:10.1186/1748-5908-6-42.
NHS England (2019) The NHS Long Term Plan. Available at: https://www.england.nhs.uk/long-term-plan/.
NHS England (2021) Green Plan Guidance for Trusts. Available at: https://www.england.nhs.uk/long-read/green-plan-guidance/.
NHS England (2023) Net Zero travel and transport strategy, in Net zero travel and transport strategy [Greener NHS]. Published 31 October 2023. Available at: https://www.england.nhs.uk/long-read/net-zero-travel-and-transport-strategy/#2-approach-and-methods
NHS England (2024) Greener NHS Strategy. Available at: https://www.england.nhs.uk/greenernhs/a-net-zero-nhs/areas-of-focus/.
NHS England (2025) Building on what we already do, in Understanding environmental sustainability [Greener AHP Hub]. Available at: https://www.england.nhs.uk/ahp/greener-ahp-hub/understanding-environmental-sustainability/building-on-what-we-already-do/
NHS England (2025) Fit for the Future: 10 Year Health Plan for England [webpage]. Published 3 July 2025. Available at: https://www.england.nhs.uk/long-term-plan/
Nicolet, J., Mueller, Y., Paruta, P., Boucher, J. and Senn, N. (2022) ‘What is the carbon footprint of primary care practices? A retrospective life-cycle analysis in Switzerland’, Environmental Health, 21:3. doi:10.1186/s12940-021-00814-y.
Pichler, P.-P., Jaccard, I., Weisz, U. and Weisz, H. (2019) ‘International comparison of health care carbon footprints’, Environmental Research Letters, 14(6). doi:10.1088/1748-9326/ab19e1.
Public Health (2024) ‘Hospitals’ contribution to health sector emissions: a systematic review’, Public Health, 232, pp. 74–86. doi:10.1016/j.puhe.2024.01.002.
RIBA (2021) Opportunities for health design research: Ab Rogers Living Systems. Available at: https://www.ribaj.com/intelligence/opportunities-health-design-research-wolfson-living-systems-ab-rogers
Romanello, M., Walawender, M., Hsu, S.-C., Moskeland, A., Palmeiro-Silva, Y., Scamman, D., Ali, Z., Ameli, N., Angelova, D., Ayeb-Karlsson, S., Basart, S., Beagley, J., Beggs, P. J., Blanco-Villafuerte, L., Cai, W., Callaghan, M., Campbell-Lendrum, D., Chambers, J. D., Chicmana-Zapata, V., … Costello, A. (2024) ‘The 2024 report of the Lancet Countdown on health and climate change: facing record-breaking threats from delayed action’, The Lancet, 404(10465), pp. 1847–1896. doi:10.1016/S0140-6736(24)01822-1.
Rothwell, E., Surtees, R., Allwood, D. and Gopfert, A. (2023) ‘Virtual appointments—embracing the opportunity to reduce carbon emissions mustn’t widen health inequalities’, BMJ, 381, Article p1169. doi:10.1136/bmj.p1169.
The Lancet (2024) ‘Editorial: Climate crisis and excess deaths’, The Lancet, 404(10419), p. 703. doi:10.1016/S0140-6736(24)01822-1.
van den Berg, M. (2015) ‘Health benefits of green spaces in the living environment’, Science of the Total Environment. Available at: [URL]
World Health Organisation (2025) How can health care facilities reduce their environmental footprint and contribute to more sustainable health systems?, Policy Brief 68. European Observatory on Health Systems and Policies. Published 8 July 2025. Available at: https://eurohealthobservatory.who.int/publications/i/how-can-health-care-facilities-reduce-their-environmental-footprint-and-contribute-to-more-sustainable-health-systems
On International Women’s Day, we shine a spotlight on the incredible women at the Institute of Global Health Innovation (IGHI) who are shaping the future of healthcare worldwide. From pioneering research to innovative policy work, these leaders are tackling some of the most pressing global health challenges —making a real difference in in the UK and beyond.

In this blog, we celebrate their achievements and highlight how their expertise and dedication continue to inspire change. Read on to learn about some of these fantastic women at the IGHI and discover key examples of their work.
Professor Bryony Dean Franklin – Visiting Professor at IGHI
 Professor Bryony Dean Franklin is visiting Professor in the Department of Surgery and Cancer at the Centre for Prevention and Management at Imperial College. She is Director of the National Institute for Health Research (NIHR) North West London Patient Safety Research Collaboration (NWL PSRC), leading research in medication patient safety and the safe use of technology.
Professor Bryony Dean Franklin is visiting Professor in the Department of Surgery and Cancer at the Centre for Prevention and Management at Imperial College. She is Director of the National Institute for Health Research (NIHR) North West London Patient Safety Research Collaboration (NWL PSRC), leading research in medication patient safety and the safe use of technology.
Professor Franklin is widely recognised as a research leader within patient safety, both nationally and internationally. She has specific expertise in evaluating technologies that aim to reduce medication errors in both primary and secondary care. She led a recent revision of the World Health Organization’s Medication Safety Curriculum Guide and has recently contributed to collaborative research and quality improvement studies in Brazil, India and Finland. As Co-Editor-in-Chief of the journal BMJ Quality and Safety she seeks to support and encourage others in publishing high-quality research and opinions that seek to improve patient care the world over.
Jennifer Bennett – Senior Postgraduate Administrator
 Jennifer Bennett is a Senior Postgraduate Administrator for the PG Dip and MSc Digital Health Leadership (DHL) Programmes. She is responsible for the day-to-day administration of the programmes, supporting the students from recruitment to award and all the processes in between, working closely with faculty and teaching fellows to make sure the students get the best academic and pastoral support.
Jennifer Bennett is a Senior Postgraduate Administrator for the PG Dip and MSc Digital Health Leadership (DHL) Programmes. She is responsible for the day-to-day administration of the programmes, supporting the students from recruitment to award and all the processes in between, working closely with faculty and teaching fellows to make sure the students get the best academic and pastoral support.
Jenny gained a new perspective on the student experience last year when she completed a L3 Team Leader qualification (CMI). She particularly enjoyed learning about leadership and communication models and evaluating how she could apply them to her work. This echoes the workplace assessments which the PG Dip students are doing, applying theory to practice. The PG students on the DHL programmes are all balancing work, study and personal or family commitments and Jenny has even greater empathy for students with looming deadlines! She is pleased to have achieved a Distinction. One of the projects she reflected on was the 2024 refurbishment of the office environment of 1070 at QEQM which has become a more inviting space for collaboration with colleagues.
Recently Jenny has introduced some processes to streamline the administration of benchmarking assessments and bulk uploading feedback to the VLE. She is also looking forward to contributing on further working parties to identify Imperial’s new VLE.
Melanie Leis – Director of Policy and Analysis
 Melanie Leis is the Director of Policy and Analysis of the Centre for Health Policy, part of the IGHI. She leads the Centre’s development of analytics tools and policy outputs to support global decision-makers in fields such as patient safety, digital health and mental health.
Melanie Leis is the Director of Policy and Analysis of the Centre for Health Policy, part of the IGHI. She leads the Centre’s development of analytics tools and policy outputs to support global decision-makers in fields such as patient safety, digital health and mental health.
Melanie leads our partnership with WHO’s Global Patient Safety Collaborative, which provides an opportunity to develop global and country-specific patient safety leadership support and resources. She also leads our collaboration with the charity Mental Health Innovations to deliver policy reports that highlight the key role that digital mental health services play in supporting the UK population. One of the projects she is most proud of is the collaboration with the charity Patient Safety Watch, through which IGHI produces reports on the national and global state of patient safety. The annual launch events of the reports bring together national and global patient safety leaders, including patients. These reports and events ensure that patient safety is at the top of system leaders’ agendas.
Jodie Chan – Public Involvement Officer, Helix Centre
 Jodie Chan is a Public Involvement Officer at the IGHI’s Helix Centre, working on projects around safely involving women experiencing homelessness in research, understanding the mental health experiences and support needs of 10- to 13-year-olds, and analysing the impact of long waiting times on patients and the health system.
Jodie Chan is a Public Involvement Officer at the IGHI’s Helix Centre, working on projects around safely involving women experiencing homelessness in research, understanding the mental health experiences and support needs of 10- to 13-year-olds, and analysing the impact of long waiting times on patients and the health system.
Jodie works across IGHI to support the meaningful involvement of patients, carers, and public members in research. Within her work, she has a strong focus on deepening and diversifying IGHI’s relationships with its local community and is passionate about supporting community-led research.
She is particularly proud of the relationships she has built with women at the Marylebone Project, a local women’s homelessness service, and of their ongoing work to make research safer and more psychologically informed.
Jessica Shields – Impact Officer, Helix Centre
 Jessica Shields is an Impact Officer at the IGHI’s Helix Centre, working across the Centre to keep it running smoothly. Jess works on everything from supporting the scaling up of Helix projects and looking for funding opportunities to communications and coordinating Helix events. Jess also co-chairs the IGHI Wellbeing Working group, heading iniatives to improve workplace wellbeing at IGHI.
Jessica Shields is an Impact Officer at the IGHI’s Helix Centre, working across the Centre to keep it running smoothly. Jess works on everything from supporting the scaling up of Helix projects and looking for funding opportunities to communications and coordinating Helix events. Jess also co-chairs the IGHI Wellbeing Working group, heading iniatives to improve workplace wellbeing at IGHI.
Jess is proud to support the Helix team to bring design to healthcare and being involved in the Wellbeing Working Group at IGHI. A particular highlight has been bringing the Helix team together over games and food for the Christmas All-Staff meeting and supporting team members to find funding for projects they’re passionate about.
Dr Jang Ah Kim – Lecturer at the Hamlyn Centre

Dr Jang Ah Kim is a Lecturer at the Hamlyn Centre for Robotic Surgery, Department of Mechanical Engineering. She is interested in researching multidisciplinary approaches to understanding and controlling the interactions between materials and their surrounding environments at the micro/nanoscale. By leveraging this knowledge, she aims to develop innovative and highly precise, minimally invasive strategies for biomedical sensing and robotics, addressing challenges unique to these scales.
The mini lab (micro-nano innovation lab) that Dr Kim leads is built on the belief that big breakthroughs start small. The lab focuses on micro and nano-scale engineering, exploring how light and other physical stimuli interact with materials to push the frontiers of biomedical sensing, soft robotics, and healthcare technologies. The name mini lab itself reflects this vision—written in lowercase to symbolise its commitment to micro/nano-scale research and precision-driven, minimally invasive healthcare solutions, where even the smallest changes can lead to transformative impact. Through this work, Dr Kim and her team strive to bridge fundamental science with real-world applications, advancing the next generation of biomedical engineering solutions.
Although newly established in September 2023, the mini lab has already embarked on exciting foundational research in manipulating micro/nanoparticles and bacterial swarms using light, as well as engineering shape-changing microrobots. These efforts aim to lay the groundwork for novel applications in personalised medicine, such as targeted drug delivery, cellular-level surgery, and local immunotherapy. In the long run, these highly targeted and efficient biomedical solutions could also contribute to addressing broader clinical challenges, including optimising therapeutic strategies and reducing unnecessary antibiotic use, ultimately supporting efforts to tackle antimicrobial resistance—all of which resonate with IGHI’s vision for advancing global healthcare innovation.
Dr Ana Cruz Ruiz — Project Manager, Hamlyn Centre
 Dr Ana Cruz Ruiz is the Project Manager at the Hamlyn Centre for Robotic Surgery, where she coordinates centre-wide projects across various Technology Readiness Levels, ranging from basic research to medtech translation initiatives. In addition to this role, she leads the Hamlyn Centre’s Global Surgery working group, which focuses on how frontier technologies—such as AI, robotics, 3D printing, and the Internet of Things—can enhance surgical care in low- and middle-income countries.
Dr Ana Cruz Ruiz is the Project Manager at the Hamlyn Centre for Robotic Surgery, where she coordinates centre-wide projects across various Technology Readiness Levels, ranging from basic research to medtech translation initiatives. In addition to this role, she leads the Hamlyn Centre’s Global Surgery working group, which focuses on how frontier technologies—such as AI, robotics, 3D printing, and the Internet of Things—can enhance surgical care in low- and middle-income countries.
One of her recent achievements includes organising the Global Surgery Forum at the Hamlyn Symposium 2024, where she co-moderated a panel with Dr Kee Park, Director of Policy & Advocacy at Harvard Medical School. The session, titled “Can Technology and Innovation Help Improve Health Equity?”, addressed the challenges faced by low- or middle-income countries in accessing safe, affordable surgical and anaesthesia care. The panel explored how technology is already helping to address some of these barriers, while also emphasising the need for further collaboration with the engineering community to create scalable solutions.
Ana is passionate about improving health equity in Honduras and in Latin America. Recently, she travelled there to meet with local surgeons, learn about regional needs, and explore ways to collaborate on making surgical care more accessible. She also contributes as a member of the Advisory Council for Honduras’ 2026 National Human Development Report, organised by the United Nations Development Programme.
Georgia Butterworth – Senior Strategy Advisor to Lord Darzi
 Georgia Butterworth is a Senior Strategy Advisor to Lord Darzi, supporting the delivery of his wide-ranging portfolio across academic, policy and parliamentary priorities. In this role, she provides strategic advice and coordination across a diverse range of projects, from the Fleming Initiative to the NHS Independent Investigation. Her work is dynamic and varied, often requiring close collaboration with colleagues across the IGHI to ensure alignment across its centres.
Georgia Butterworth is a Senior Strategy Advisor to Lord Darzi, supporting the delivery of his wide-ranging portfolio across academic, policy and parliamentary priorities. In this role, she provides strategic advice and coordination across a diverse range of projects, from the Fleming Initiative to the NHS Independent Investigation. Her work is dynamic and varied, often requiring close collaboration with colleagues across the IGHI to ensure alignment across its centres.Jessica Newberry Le Vay – Climate Change and Health Policy Fellow
 Jessica Newberry Le Vay is a Climate Change and Health Policy Fellow in the Climate Cares Centre, working on the interconnections between climate change and mental health. Jess recently worked on the Connecting Climate Minds Global Research and Action Agenda, bringing together the perspectives of 960 experts across 100 countries to set out global priorities for climate change and mental health research and a vision for implementing and translating that research to action. Jess was also recently part of developing the People’s Petition, a global collective climate justice call submitted to the International Court of Justice in December 2024 that amplifies the testimonies of 18 witnesses from communities experiencing and responding to the worst impacts of the climate crisis, including impacts to physical and mental health.
Jessica Newberry Le Vay is a Climate Change and Health Policy Fellow in the Climate Cares Centre, working on the interconnections between climate change and mental health. Jess recently worked on the Connecting Climate Minds Global Research and Action Agenda, bringing together the perspectives of 960 experts across 100 countries to set out global priorities for climate change and mental health research and a vision for implementing and translating that research to action. Jess was also recently part of developing the People’s Petition, a global collective climate justice call submitted to the International Court of Justice in December 2024 that amplifies the testimonies of 18 witnesses from communities experiencing and responding to the worst impacts of the climate crisis, including impacts to physical and mental health.
Jess currently leads The Compass Project: Guiding minds and inspiring action through climate change education, working with young people and educators in schools and universities to ensure climate change education can equip and support young people with the resilience, knowledge, skills and agency to take climate action and live in an uncertain future.
Dr Emma Lawrance – Climate Cares Centre Lead
 Dr Emma Lawrance is the Climate Cares Centre Lead and Mental Health Lead at the IGHI. Emma also leads the Wellcome-funded global initiative Connecting Climate Minds, which has involved over 1000 people across 100 countries to date. She holds an AXA Climate and Health Fellowship to more deeply understand the experiences of young people in the climate crisis in different cultures, what this means for their mental health and wellbeing, and to co-design and evaluate support that can build agency and resilience.
Dr Emma Lawrance is the Climate Cares Centre Lead and Mental Health Lead at the IGHI. Emma also leads the Wellcome-funded global initiative Connecting Climate Minds, which has involved over 1000 people across 100 countries to date. She holds an AXA Climate and Health Fellowship to more deeply understand the experiences of young people in the climate crisis in different cultures, what this means for their mental health and wellbeing, and to co-design and evaluate support that can build agency and resilience.
Emma is a recognised global leader in the emerging climate and mental health field, building awareness and capacity across sectors and countries to acknowledge and act for a climate of health and wellbeing. She is an author of key research and policy papers on the topic, including: the first global policy brief; leading reviews of the field as a whole, relevant interventions, and temperature and mental health; studies with young people in the UK, Caribbean and the US (under review), and the Global Research and Action Agenda for climate change and mental health. She has presented globally, for instance at the World Economic Forum, four UNFCCC COP conferences, the World Congress of Psychiatry, OECD and the European Commission and been featured in international media, including Die Zeit, Guardian, Al Jazeera, Sky News, BBC, Forbes, Reuters and others.
She believes in the power of community, and in connecting people and ideas to foster resilience to thrive in a changing world and to create a safer climate for our mental health.
Dr Laura-Maria Horga – Communications and Events Officer
 Dr Laura-Maria Horga is a Health Communications and Events Officer at IGHI. She delivers communications and engagement projects across IGHI’s seven research centres of excellence, supporting the Institute’s mission to tackle global health challenges.
Dr Laura-Maria Horga is a Health Communications and Events Officer at IGHI. She delivers communications and engagement projects across IGHI’s seven research centres of excellence, supporting the Institute’s mission to tackle global health challenges.
Laura has contributed to key projects, including the National State of Patient Safety Report 2024, which gained prominent media coverage for highlighting critical maternity care issues; the Mental Health Innovations Report, which explores digital solutions to meet growing mental health needs (Shout service); the Great Exhibition Road Festival; the Julia Anderson Training Programme; Connecting Climate Minds; the Digital Health Leadership Programme; and many others.
She is currently leading the organisation of IGHI’s annual in-person event, Demo Day, which helps staff learn more about the different workstreams at IGHI, connect with colleagues, foster collaborations, and celebrate the Institute’s achievements.
Laura is also a certified Mental Health First Aider at Imperial College London.
Dr Ivet Angelova – Research Associate
 Dr Ivet Angelova has recently joined the MedTechOne programme at Imperial College London as a MedTech Specialist. Her journey into healthtech began with a PhD in Chemical Engineering, where she focused on developing genetically encoded biosensors for monitoring Botulinum Neurotoxins—a project that deepened her passion for turning scientific discovery into practical healthcare solutions.
Dr Ivet Angelova has recently joined the MedTechOne programme at Imperial College London as a MedTech Specialist. Her journey into healthtech began with a PhD in Chemical Engineering, where she focused on developing genetically encoded biosensors for monitoring Botulinum Neurotoxins—a project that deepened her passion for turning scientific discovery into practical healthcare solutions.
Shaping the future of healthcare means not only driving research and innovation but also ensuring it reaches those who need it most. As part of MedTechOne, Ivet is currently working towards building a knowledge base that equips early career researchers (ECRs) with the tools to translate medtech discoveries into real-world impact. This resource is shaped by the needs and feedback of researchers across IGHI, the Hamlyn Centre and the wider Imperial community. Covering everything from regulations and quality standards to commercialisation and team building, this resource is designed to help bridge the gap between research and commercialisation. Additionally, she is co-leading the launch of the MedTech ECR Network at Imperial, creating a space for emerging medtech leaders to connect, collaborate, and thrive.
Ivet said “This International Women’s Day is a chance to celebrate the women driving healthcare forward, breaking barriers, and shaping a future where innovation is inclusive, impactful, and accessible to all. I am grateful to be part of a community filled with inspiring women whose work and determination continue to push the boundaries of what is possible in medtech and beyond.”
Cohort 7 Trainees – Julia Anderson (JA) Training Programme
 Caitlin Murphy is as a JA Behavioural Science Trainee in the Fleming Initiative team. She is working in a patient / public facing project focusing on the use of antibiotics and encouraging individuals to finish a course of antibiotics if prescribed.
Caitlin Murphy is as a JA Behavioural Science Trainee in the Fleming Initiative team. She is working in a patient / public facing project focusing on the use of antibiotics and encouraging individuals to finish a course of antibiotics if prescribed.
Arlette Albert is another JA Behavioural Science Trainee in the Fleming Initiative team. She is working part-time alongside Caitlin to develop her skills in qualitative research, behavioural science, patient engagement, and co-designing interventions.
Miranda Watson joined as the JA Trainee in Digital Health. She is working in the Patient Safety team to develop her skills in translating evidence into measurable interventions to improve patient safety in virtual care. She is involved in reviewing the literature, extracting data, and critically appraising available literature to identify safety indicators relevant to virtual consultations.
Last week, over 100 students from the most recent Cohort of the Digital Health Leadership Programme (DHLP) came together for the first time to kick off their learning journey.

The two-day Forum in York gave students the opportunity to learn about expectations for the year, meet the academic team, and network with peers. Day 1 included talks and interactive sessions on individual strengths, while Day 2 focused on the collective, with participants engaging with their peer support groups.
Commissioned by the NHS Digital Academy at NHS England, the DHLP empowers health and care leaders to drive digital transformation in the NHS. The programme is delivered by a partnership of Imperial College London’s Institute of Global Health Innovation, HDR UK and Imperial College Healthcare NHS Trust. The programme is targeted at individuals who are working in a role where they are required to drive and implement practical digital transformational change within their organisation or system.
Now in the seventh year of delivering the programme, we are pleased to be onboarding a diverse cohort of digital leaders and aspiring ones across the health and care spectrum. This includes an equal split between clinical and non-clinical digital roles, with good representation across midwifery, nursing, pharmacy, AHPs and other medical professions.
In this blog post, Cohort 7 students shared their motivations for applying for this programme and what they think the impact will be, as well as their impressions about the event.
 ‘’I joined this programme to expand my knowledge in the digital health field, grow my network, and learn something new that I can apply in my organisation and the wider community. I aim to transfer that knowledge to my colleagues, or at least have them feel my impact in some way.
‘’I joined this programme to expand my knowledge in the digital health field, grow my network, and learn something new that I can apply in my organisation and the wider community. I aim to transfer that knowledge to my colleagues, or at least have them feel my impact in some way.
‘’As part of this event, we’re learning new things about ourselves—as managers, as leaders—and discovering what we need to do to become better people.’’
 ‘’I have the opportunity to be a great contributor in my team, so I need to upskill myself, my leadership skills, especially around digital landscape.
‘’I have the opportunity to be a great contributor in my team, so I need to upskill myself, my leadership skills, especially around digital landscape.
‘’These two days have been really empowering. Meeting my peers and the teaching fellows ignited my passion to be a great leader and bring about changes in the digital landscape and the NHS. I’m very happy to have each of my peers in the different groups. we have many different opinions, which I appreciate, as I enjoy being challenged with my ideas.’’
‘’I completed the Postgraduate (PG) Certificate in Digital Maternity Leaders previously and now progressed to the PG Diploma. I was seeking further training and community for clinicians who found themselves in similar roles to mine, to support my work and gain more knowledge.
‘’My original training was as a midwife, not in digital health, so I found myself in this niche of healthcare that I really enjoy and want to learn more about to see what the impact is.’’
 ‘’I can absolutely see how the data and systems we use within the workforce haven’t caught up with the rest of the digital world. So, I’m hoping to gain from this course not only opportunities to enhance my leadership skills and support my career development, but also to advance the workforce systems and help our diagnostics staff become more digitally enabled and ready for the future.
‘’I can absolutely see how the data and systems we use within the workforce haven’t caught up with the rest of the digital world. So, I’m hoping to gain from this course not only opportunities to enhance my leadership skills and support my career development, but also to advance the workforce systems and help our diagnostics staff become more digitally enabled and ready for the future.
‘’Since I had to defer for a year, I was very impressed by how supportive the team was when I wanted to start again this year. The Forum today has been outstanding, and I am thrilled to be here!’’
 ‘’I’ve taken on some more senior leadership roles in digital, and I felt I needed to gain more expertise to perform better in those roles. I decided to come to Imperial to do that, and to translate that learning into tangible outcomes and see effective change happen in the organisation I work for.
‘’I’ve taken on some more senior leadership roles in digital, and I felt I needed to gain more expertise to perform better in those roles. I decided to come to Imperial to do that, and to translate that learning into tangible outcomes and see effective change happen in the organisation I work for.
‘’It’s been great meeting others in the cohort and the new peer support group I’ll have this year. I’m sure there will be some ups and downs that we’ll need to support each other through.
‘’My favourite session was the strengths assessment. It emphasised the importance of viewing yourself not through a deficit lens, but rather through a positive perspective on what can be improved. Using your natural talents and strengths can help in areas of your life where you don’t feel as strong, which I find quite pivotal.’’
 ‘’I would like to gain an academic understanding of the programme and how we apply clinical informatics in the broader AHP-related field. Being appointed as the first Chief AHP Information Officer has provided me with the platform to raise the profile of AHPs within the digital agenda across the NHS, so I am motivated by this.
‘’I would like to gain an academic understanding of the programme and how we apply clinical informatics in the broader AHP-related field. Being appointed as the first Chief AHP Information Officer has provided me with the platform to raise the profile of AHPs within the digital agenda across the NHS, so I am motivated by this.
‘’It’s fantastic to meet all the colleagues who have joined the program, as well as the academic staff. I am impressed with the facilities here and how organised and supportive the team is!’’
 ‘’I’ve been involved in many digital health projects in my Trust, and I’m eager to improve stakeholder engagement and collaboration among executive teams, clinical teams, and IT to effectively deploy digital health systems.
‘’I’ve been involved in many digital health projects in my Trust, and I’m eager to improve stakeholder engagement and collaboration among executive teams, clinical teams, and IT to effectively deploy digital health systems.
‘’Networking with like-minded people in different roles has been the best part for me. I believe this can drive change and facilitate knowledge sharing across the NHS, helping us work collaboratively instead of in silos. That’s how we can learn from each other and accelerate progress in digital health for the UK and NHS. The insights on leadership styles, CliftonStrengths, and the reflective learning session were particularly valuable to me.’’
 ‘’I work in primary care in an area of high social deprivation in the UK. When you work in a place with such deep need, digital change is one of the obvious equalizers. But how do you make that happen? I’m here to understand what we need to do better to implement change at the ground level.
‘’I work in primary care in an area of high social deprivation in the UK. When you work in a place with such deep need, digital change is one of the obvious equalizers. But how do you make that happen? I’m here to understand what we need to do better to implement change at the ground level.
‘’What I saw happening today was many people making an effort to go beyond speaking with those they already knew or had sat next to. This created a really convivial vibe, which was great for setting up peer groups. That’s one of the most inspiring things I’ve noticed—how the learning over the last six cohorts has allowed this to happen fairly organically.’’
 ‘’My first motivation is engaging with more people from different backgrounds, from clinical to project management. My second motivation is gaining hands-on experience rather than just theory. Third, I am interested in learning and stepping out of my comfort zone.
‘’My first motivation is engaging with more people from different backgrounds, from clinical to project management. My second motivation is gaining hands-on experience rather than just theory. Third, I am interested in learning and stepping out of my comfort zone.
‘’I want to get the most out of this course and apply the principles I learn here both in my personal life and within my team. I believe that if I don’t change, nothing will change.
 ‘’I was looking for something that would impact my work and challenge me on different levels. After the last two days, I am certain that’s exactly what I will get. The past two days have been intense, giving me lots of stimuli and challenges—all the things I was hoping for. I hope this will continue for the next 12 months.
‘’I was looking for something that would impact my work and challenge me on different levels. After the last two days, I am certain that’s exactly what I will get. The past two days have been intense, giving me lots of stimuli and challenges—all the things I was hoping for. I hope this will continue for the next 12 months.
‘’The insights from the strengths assessment have definitely been a key highlight for me. I believe that’s a ‘gift’ that will continue to provide value, a resource to go back to and learn from, offering ongoing reflections.‘’
Find out more about the Digital Health Leadership Programme, and read about the programme accreditation with the Federation for Informatics Professionals in Health and Social Care.
“Arca sull’albero”, a new children’s hospice in Bologna, Italy, was inaugurated last week, marking a significant milestone in children’s palliative care. The hospice, funded by Fondazione Hospice Maria Teresa Chiantore Seràgnoli, is a testament to innovative, user-centred design and care. Researchers and designers from the Institute of Global Health Innovation (IGHI) and its Helix Centre played a pivotal role in its development, ensuring the incorporation of lessons from international best practices and of user-centred innovation.

Access to children’s palliative care is a human right. According to the United Nations Committee on the Rights of the Child, “children are entitled to quality health services, including prevention, promotion, treatment, rehabilitation and palliative care services.’’ However, 8 million children around the world need specialist palliative care, but only 10% of them actually receive it. Even in otherwise developed health systems like Italy’s, provision of paediatric palliative care is limited.
“Arca sull’albero” is one of the first and most innovative children’s hospices in Italy. It stands out as unique in several key ways. Its architecture, designed by Renzo Piano Building Workshop, merges functionality with a serene, home-like atmosphere, providing a comforting sanctuary with natural light and open spaces.

The hospice’s care protocols align with global best practices, ensuring the highest standard and continuity of care. Focus on user experience is paramount, with every detail meticulously designed to make the stay comfortable and stress-free for children and their families. Additionally, the hospice’s governance and management processes aim to maximise effectiveness and openness to innovation.
Isabella Seràgnoli, from the Fondazione Hospice Maria Teresa Chiantore Seràgnoli, said:
“The children’s hospice represents concretely the concept of care. Palliative care is not only about treating physical pain, but also psychological pain, and requires attention to the situation of the person and their family. For this reason the hospice is an open and permeable place, a home where social relations and affection are possible and in which to experience beauty.’’
The IGHI team has been involved from the project’s inception. Leveraging its extensive expertise and research, IGHI informed the hospice’s strategy and its approach to innovation, ensuring that “Arca sull’albero” not only meets but exceeds global standards in children’s palliative care.
Designers from the Helix Centre engaged with children and their families, including siblings, to understand their needs and put them at the centre of IGHI’s research efforts in this area. They also designed prototypes of innovative solutions that informed the plans of Fondazione Hospice Maria Teresa Chiantore Seràgnoli for the new hospice.
Gianluca Fontana, Deputy Director of IGHI, said:
“It is rare to be able to play an active role in the creation of a new healthcare provider. I am proud of the work of many IGHI team members in researching and designing solutions in children palliative care. I am extremely grateful to Fondazione Seràgnoli for the trust they put in us and for their support of our activities in this space.”
A team from IGHI’s Centre for Health Policy led the development of the report, “The children’s palliative care provider of the future: A blueprint to spark, scale and share innovation”. The report emphasises the importance of innovation in children’s palliative care, advocating for adopting new technologies, interdisciplinary collaboration, and a patient-centred approach. Through interviews with 51 experts in 27 countries, the project identified 9 key features of innovative paediatric palliative care providers:
“Arca sull’albero” exemplifies these characteristics, setting a new standard for children’s hospices in Italy and beyond. The report also revealed the opportunity for dedicated advancement of excellence and innovation in paediatric palliative care worldwide. With the support of the partnership between Fondazione Hospice Maria Teresa Chiantore Seràgnoli and the Institute of Global Health Innovation, Global Treehouse Foundation was established and is now working in partnership with innovators, funders, providers and entrepreneurs to address the global lack of access to children’s palliative care.
Laura Dale-Harris, Founder Director of Global Treehouse Foundation, added :
“Arca sull’albero is a model of where the global children’s palliative care field can grow – deep local roots with families, children, and communities – partnered with innovators and expertise like IGHI. We are excited to welcome Arca sull’albero to the community of entrepreneurial children’s palliative care providers around the world.”
At the inauguration last week, Gianluca Fontana from IGHI took part in an event alongside Renzo Piano, the building’s renowned architect, paediatric palliative care experts Professor Julia Downing, CEO of the International Children’s Palliative Care Network, and Dr Renee McCulloch from Great Ormond Street Hospital and University College London. The speakers presented the latest development in paediatric palliative care globally to an audience of paediatricians and nurses from the Emilia Romagna region.

Renzo Piano described his vision for the architectural project, an “ark on the trees where children and families can find relief surrounded by the magic and natural beauty of the woods”. Professor Downing presented a global overview of the development of paediatric palliative care services. Dr McCulloch shared her experience working in research and clinical practice in the sector. Gianluca Fontana spoke about the key features of the paediatric palliative care provider of the future.

IGHI is committed to improvement and innovation in paediatric palliative care and in the health of children more broadly. Beside the continued collaboration with Arca sull’albero and Global Treehouse Foundation, researchers at IGHI and Helix have a number of early stage projects working with children and young people, particularly around mental health and rare diseases, for which they are interested in exploring opportunities for further collaboration and funding.
In February we hosted the Julia Anderson Training Programme (JATP) Careers Event 2024 at Institute of Global Health Innovation (IGHI), a fantastic evening for sixth form students to learn more about our Julia Anderson programme and the IGHI, and get inspired for their future careers.

Sixth formers from different London state-funded schools travelled to The Invention Rooms, at Imperial College London’s White City Campus, to participate in the event. They got the chance to learn more about the opportunities at IGHI, hear some of our staff members’ career journeys, as well as interact with some of the fantastic workstreams we work on to improve people’s health.
About the Julia Anderson Programme and next cohort recruitment
The evening started with Sophie Pieters, IGHI Operations Officer and JATP Programme Lead, welcoming the attendees and introducing the JATP programme, including the eligibility criteria and the new trainee roles available in the summer.
The Julia Anderson Training Programme gives people with limited or no work experience the opportunity to join an impactful stream of work at IGHI, Imperial College London’s. The paid programme gives trainees the opportunity to grow their network, boost their CV and develop applicable workplace skills and knowledge.
Sophie announced the three upcoming roles for the next cohort in July, specifically Analytics and Events Trainee, Public Involvement Trainee and Educational Research Trainee (the first two are open to those with no university). On 14 March, a webinar will be held to provide people with more information on the programme, the training positions on offer and useful advice for the application. Students were highly encouraged to sign up for the webinar.
Career talks from IGHI staff and trainees
Next, some of the IGHI staff and current trainees delivered individual presentations highlighting their career journey, challenges, and other valuable insights from their experience.
“I found the job I loved although didn’t know it existed. It’s okay if you don’t know what you want to do.’’, said Eleni Daniels, Patient Safety Research Centre (PSTRC) Manager at IGHI, who has a background in biomedical sciences and worked in advertising before finding her dream job in a patient safety field.

Amish Acharya, Scientific Advisor to Professor Ara Darzi at IGHI, talked about his ‘unconventional’ career path from medicine, followed by PhD in Behavioural Science, to his current role, where he is contributing to creating research projects and supporting the progress of scientific work. Amish advised:
“Exams don’t represent who you are and what you can do. It’s never too late to change your path, don’t be afraid to try different things – this can often make you more adaptable and rounded as a person.’’
One of our current Julia Anderson Trainees, Tania Domun, a graduate of Population Health and Medical Sciences with a Master’s degree in Public Health, shared her experience so far as a JATP trainee in Behavioural Science and the benefits of joining the programme:

“JATP allows you to develop your skills and support you with the next steps in your career. It’s challenging when you don’t have a mentor or people to help you navigate your professional path. The programme does exactly that, by focusing on you as an individual. It’s a lot about your passions and not your previous work experience. This makes it a unique programme.’’
She also talked about the Imposter syndrome: ‘’I’ve realised many people, including me, deal with this syndrome – don’t let these feelings stop you from applying for the programme. This is the best time to explore possibilities and build new skills.’’
Lastly, Clarissa Gardner, Senior Design Researcher at TPXimpact and Honorary Research Fellow, spoke about her career journey as a ‘learning process’ and how she came about setting the JATP programme, after doing a MSc in Health and Design at IGHI:
‘‘Your job title doesn’t matter as much as your ability to help others and inspire positive change. I recognised the diversity of people at IGHI, so I proposed this programme to create work experiences for people.’’
Interactive activities showcasing IGHI Centres’ work
After these inspiring talks, we organised interactive activities led by each of the IGHI Centres. During these sessions, attendees had the opportunity to engage with the different workstreams at IGHI in small groups and interact with IGHI staff members.
The Hamlyn centre hosted a ‘create your own surgical robot’ activity. Sixth formers were challenged to conceptualise the design of a robot, then turn their drawings into 3D images using specialised software. Hamlyn centre representatives also explained the benefits of surgeons using surgical robots compared to traditional surgery methods, highlighting how they enhance precision during procedures. The participating team included Brandon Davies, Learning Technologist, Nazia Bharde, Project Officer, Robert Merrifield, Medical Design Associate and Salzitsa Anastasova-Ivanova, Facilities Manager.

At one of the Helix Centre stands led by Jodie Chan, Patient and Public Involvement and Engagement Officer, and Clare McCrudden, Policy Fellow from the Change Lab, students had the opportunity to discover how the public can influence research priorities, methodologies, and dissemination for healthcare improvement. They were encouraged to brainstorm alternative names for ‘antimicrobial resistance’ and open the ‘can of worms’ around healthcare data through an interactive activity, sparking further discussions on its benefits and risks.

They also learned about one of the upcoming JATP roles – Public Involvement Trainee – who will help to involve local youth groups and schools in a project aimed at better understanding the mental health needs of children across the UK and identifying how services can better support them.
The second Helix Centre stand was led by Matthew Harrison, Senior Design Associate, Alex Dallman-Porter, Designer Healthcare Products, and current JATP trainee, Andrew Watt. People were invited to participate in a grip strength assessment activity, during which they were asked to squeeze a ball-shaped dynamometer (‘squegg’) in their hand to measure their frailty levels and compare with their peers. Additionally, the stand showcased a sleeping mat used for measuring heart rate and respiratory rate, along with other environmental sensors designed for individuals with dementia.
Jessica Newberry Le Vay, Climate Change and Health Policy Fellow at the Climate Cares Centre, hosted an interactive session about exploring climate emotions and imagining what future they want to see. The students were challenged to think about the following questions: ‘’How does climate change make you feel?, What stories do you hear about the future?, What would you want the future to look like?’’
People were able to discuss their responses to these questions and see what other people have put. They explored actions that can improve both mental health and the climate, building hopeful and constructive narratives around climate change.
Eleni Daniels from PSRC also had a stand on patient journey. She encouraged students to reflect on healthcare experiences of themselves, their family members, or friends, and to consider how these experiences could be further improved. People shared their thoughts and experiences, engaging in a dialogue that allowed them to open up and explore patient journeys from the GP to hospital settings.
Feedback from sixth formers
We were impressed by the amount of positive feedback we received from the sixth formers. Some examples below:
“I’ve discovered that you don’t need to know exactly what you want to do at this age. It’s more important to be open to learning and taking on new opportunities and experiences.”
“Many internships and training programmes require individuals to meet specific minimum requirements. It’s fantastic to discover that the JATP program doesn’t have such requirements, giving people the chance to gain those skills and build experience.”

“I found the event very engaging and fun. It made me think about my future career, the steps I want to take next and the sort of support I should be seeking. I am keen to apply for this programme!’’
On the day feedback indicated that, among our participants, 90% were inspired for their career after attending the event. According to our post-event online survey, 92% of our participants expressed their willingness to recommend JATP to a friend, while 83% of respondents indicated their intention to apply for JATP in the future.
We are looking forward to seeing people applying for the JATP programme and taking advantage of the tremendous opportunities at IGHI to advance in their careers. The event was made possible by the EDI Seed Fund and we are very grateful for their support.
On your marks, get set… Our MSc Healthcare and Design students take part in a Design Dash, a rapid design process to solve a real-world healthcare challenge. We spoke to two students, Aoife McGrath and Jasmine Banerjee, about the process.
A design dash is a rapid, collaborative method for conceiving tangible healthcare innovations. Our Helix Centre teaches and assesses the Design Dash module on the MSc Healthcare and Design course that is aimed at healthcare professionals and designers and co-run by Imperial College London and the Royal College of Art. The students work with Helix Centre’s researchers, designers and public engagement experts on a live rapid design project to prototype a solution to an identified challenge.

This year, the Design Dash focused on NHS screening programmes for cancer, which are important for both patients and the NHS, as detecting cancer early gives people a better chance of responding to treatment and therefore recovering from their illness.
The module starts with an action-packed week running through the Design Dash process, offering a chance to explore a new brief in an intense, collaborative and open-minded way. With an initial focus on bowel cancer screenings, the students were taken through the process of framing and dissecting briefs and understanding patients’ experiences. After the group projects, the individual assignment for the module was to create a project to increasing the uptake of breast or cervical screening.
While the end products of the Design Dash are only prototypes, by applying real-world design techniques that Helix Centre uses, the students gain knowledge that will stay with them throughout their careers.

I’ve come straight onto this master’s from doing an undergraduate in product design. I have a keen interest in medical technology and focused on this for all my undergraduate self-led projects.
The Design Dash week was fantastic, well organised and the content was brilliant. It was set up really well to teach us about important considerations for any design project, particularly for the students from a non-design background, such as by creating ‘how might we’ questions to help guide your research.
For my assignment, I chose breast screening as I had a whole range of expert patients that I could think to talk to. I also spoke to a GP who gave their interpretation of why there was low uptake and which patients they have to chase up to attend screenings. I was aware that people from ethnic minorities were less likely to attend screenings, and I wanted to consider how to approach these women. Based upon insights from my interviews with patients and my secondary research, the main barriers I identified were access to information, knowledge of what to expect and knowledge of their local unit.
“The main barriers I identified were access to information, knowledge of what to expect and knowledge of their local unit”
People often say they don’t have time to go to their screenings or have time to learn about it. So I thought, when is the time in a person’s life when they are ‘wasting time’ but have no other option? When they’re on public transport! I started looking at statistics about how long people spend on the tube during the commute and thought that using the London Underground was a good way of targeting every demographic.
I developed the ‘Boob Tube’, which is based on the London Underground, but the idea is for each tube line to be sponsored by, or working in partnership with, a breast cancer charity such as CoppaFeel!. Each carriage is filled with child friendly and religiously sensitive infographics, containing information on breast screening, what it is, what to expect, how to prepare for it, and why it’s important.


Alongside this, a lot of the people I interviewed said they felt discomfort with the level of nudity in front of healthcare professionals. So, I designed a boob tube top, with the ‘Boob Tube’ logo, which you can whip down and back up in-between each scan.
Breast cancer is one of the most common cancers, and screenings are an important way to protect yourself, but also in a secondary way, to protect your friends and family who care for you. They are there to provide you with reassurance and give you the best chance.”

“I currently work as a Senior Microbiologist, on the development of consumer healthcare products.
The Design Dash was like a R&D sprint, from the early stage of understanding what the problem is, to creating final prototypes, all the while focusing on human-centred design. During the week, we spoke with people who had experience of bowel cancer screening, to first hand understand the concerns and feelings about the process. Getting those patients, users and experts involved from the beginning of the design process is hugely important and a key learning for designing in healthcare – you have to design with people at either end of the bell curve; you can’t just design for an average person.
“Getting patients, users and experts involved from the beginning of the design process is hugely important and a key learning for designing in healthcare”
For my own Design Dash research project, I chose to explore cervical screening, as I’m in the screening age bracket, so have first-hand experience and felt it would be easier to reach out to others. I created and shared an anonymous questionnaire, in addition to reaching out to my peers who were comfortable to speak on the subject, which enabled me to gather feedback about people’s experience with cervical screening.
A main theme identified through my research and interviews was a lack of education, people don’t fully understand why cervical screening is required or beneficial. More than one of the women I spoke to said ‘no one ever told us about this in school, we didn’t learn anything about it until I received the appointment letter in the post. Why are we not taught about this?’
There was also an issue of time, with NHS appointments typically being scheduled through the working day, resulting in people taking time off work. The subject of cervical screening or smear testing is rarely discussed, it’s a very personal topic and people don’t really talk about it. Thinking about this, other items such as sanitary products, tampons and contraception are readily available with less discomfort, but targeting the same area. Therefore, with my design, I tried to look at different aspects where I could improve three things – education, time and emotions.
My design idea was to combine cervical screening swab samples with sanitary products. The idea would help educate people, making them more aware of cervical screening, and also reducing the time it takes to currently attend a screening appointment. During the COVID-19 pandemic, we were all doing our own swab sampling – to detect the virus. The cervical screening test used to detect the human papilloma virus, which can potentially lead to cancer, so why couldn’t we do cervical screening tests at home?

I read about the ‘small c’ campaign – YouScreen, where they have piloted a study of 30,000 women in North London, to assess if they could sample at home. 99% of those women were able to successfully and collect their own cervical sample, which was brilliant. The idea is you use a normal swab and then send it off to a lab like you would for a PCR COVID test. However, I thought, the swab might be a bit awkward, so how can we make this easier? So, my idea is to use the tampon applicator to help people take the sample. A tampon is something that is part of everyday life, therefore more comfortable and perhaps doesn’t seem as foreign as a swab.
My design also raises awareness of cervical cancer, having information about the importance of the screening on the packaging, with links of how to collect a sample with the special tampon applicator. Creating a rapid screening test, like COVID lateral flow tests, would simplify this further and anytime you buy a pack of tampons you can check from the comfort of your own home. A rapid cervical screening test is not yet available, but it is feasible to get there.
Potentially this could take a burden off the NHS by reducing the amount of cervical screening tests the NHS needs to do. While also enabling the positive results to be detected sooner. It’s estimated that there has been a 70% reduction in cervical cancers from screening, but 83% of deaths could be prevented if everyone attended regularly. It’s a hugely important test to save lives, to empower women and people with a cervix to take control of their own health.
“It’s estimated that there has been a 70% reduction in cervical cancers from screening, but 83% of deaths could be prevented if everyone attended regularly.”
The Healthcare and Design course works directly with the NHS, and it’s a pivotal time to design efficient, frugal, clever solutions to help healthcare systems. Providing solutions to screenings, which prevents people from needing treatment, would be a huge help for people, but also healthcare systems in the UK and globally.”
Do you want to join us and use design thinking to solve problems in healthcare? Our MSc in Healthcare and Design is now open for applications, offering a hybrid teaching model so that you can learn flexibly at your own pace. Find out more about this course and how to apply on our website.
The Helix Centre, part of the Institute of Global Health Innovation, is helping stroke patients to manage their recovery and increase their independence, with a wearable tool that provides support for the rehabilitation of their arm and hand.

OnTrack Rehab is a platform that combines tracking of arm movements through a smart watch with personalised virtual coaching and dedicated clinical support. The system allows stroke patients to convert every-day activities into productive rehabilitation, and stroke therapists to monitor and help guide the patients’ progress. The development of the platform has been led by a multidisciplinary team at Helix including Gianpaolo Fusari (Project Lead) and Clare McCrudden (Engagement Lead). Gianpaolo and Clare recently ran a data collection experiment involving 20 stroke survivors to improve the software behind OnTrack.
Sana, a stroke survivor, volunteered to participate in this experiment, and met with us to describe her experience. Senior Occupational Therapist Simone Welch works in the stroke team at Charing Cross Hospital (Imperial College Healthcare NHS Trust), and chatted with us about the medical support for stroke survivors.
In 2021, Sana experienced weakness in her left side following a medical procedure, and ultimately was diagnosed with a stroke. “I felt lucky in my stroke – though not lucky to have a stroke! – because stroke outcomes could be more significant.”
Sana’s physical symptoms such as some limited arm movement required ongoing management and rehabilitation as well as sensory-based issues, like those of many stroke survivors. But it can be difficult for those who’ve had a stroke to know what to expect. Sana described that support came not only from her medical team, but beyond – reading information on the internet to understand her issue, and the information provided by medical charities.

During a visit to hospital, an NHS physio checked that Sana could do simple everyday tasks, like brush her hair. But at home, it was more challenging to engage with the ongoing exercises.
Sana felt that the support and rehab she needed wasn’t as easy to see as most of her impairments were more hidden and not so obvious. “I am grateful that it could have been worse but if I had something more significant and visible then people would be taking me more seriously.” So when the Stroke Association sent a physiotherapist to her house for assessment and gave her exercises it was the beginning of better support.
“When it’s painful you just don’t want to do [the exercises],” Sana said. With the difficulty of engaging with exercises, plus limited face-to-face support during the pandemic and the lack of services tailored for younger people who’ve had a stroke, tailored support is needed.
As a young person surviving a stroke, Sana wanted to see support that would allow for variabilities in age and outcome, rather than a ‘one size fits all’ approach. So the invitation to participate in OnTrack’s stroke rehabilitation was appealing. Sana felt that by participating in the research, her experience was able to help others, especially when those people did not fit the ‘usual’ stroke survivor’s demographic.
One aspect of OnTrack that Sana liked was the idea of “meaningful movements”. Physiotherapy rehabilitation requires hundreds of specific or purposeful movements each day, which felt unattainable. But with the smart-watch style device, Sana describes feeling more able to achieve goals – through every-day tasks such as brushing hair and doing dishes – which count as meaningful arm movements for rehab.
“This would have been useful to me; I need to engage with something interactive,” Sana said. That’s where the app helps – measuring activity and giving motivation/feedback reinforced through different channels within the watch and app, and through the support provided by therapists.

Sana’s message to survivors: “It does get better.” Sana recommends to engage with the exercises, and found YouTube videos and stroke support charities helpful in her recovery.

Simone first saw the OnTrack technology in its very early stages – when in-person service provision was really limited during the pandemic. “[It] provided an intervention that allowed [stroke survivors] to continue with the upper limb recovery”, said Simone, as well as to participate in research.
Within 24 hours of being admitted to the HyperAcute stroke unit where Simone works, the patient will be referred for a therapy assessment – be it speech, physical or occupational therapy. But the rehab certainly doesn’t end there. Where some boroughs have intensive community stroke therapy available, including at the patient’s own home, the vast majority of rehab happens when the patient is on their own. “There is a concept called self-management which is really, really important,” where patients take on responsibility for their progress and their rehabilitation.
Simone wants her patients to be able to be discharged and return home. And the app would really support them to be able to track how they’re doing with their arm and hand recovery when not in hospital. When stroke patients like Sana have an arm weakness, OnTrack Rehab can send reminders, and help them to focus on what they need to achieve. “So it’s a bit like a step counter for the arm,” explains Simone.
As any movement of the arm – actual exercises or using your arm to wash your face or to feed yourself – is beneficial, tracking with OnTrack is a really positive solution.
There’s plenty of hope about what OnTrack could help with. Simone said: “I think it would help guide conversations between therapist and patient on how they can do more outside of their sessions.” Plus, it gives data that therapists can go through with their patient to support them to reach their goals.
“There’s a lot you can do to support someone’s overall quality of life and their well-being”, says Simone. The app could prompt therapists to ask: “I can see you were really active at this time of the day, but not so much here – what was happening?” This is particularly important when therapists may only see their patient for an hour, as the app allows you to know what’s happening in the other 23 hours of the day.

For OnTrack Rehab, Clare and Gianpaolo are working to evaluate the device and its impact with more people and this year a new clinical trial will begin.
Gianpaolo said: “The data and insights that we gathered with the collaboration of Sana and other stroke survivors during Phase 1 has helped us to improve the OnTrack experience as a whole. One big change that we can’t wait to test during Phase 2 is the inclusion of smarter prompts delivered directly to the patient’s wrist, hopefully we will be able to see how these tailored messages motivate people to increase the use of their arm in more varied activities.”
“We are delighted to have members of the research study as part of a wider group of stroke survivors and carers guide us through the next phase of OnTrack Rehab, piloting it in the NHS. We expect to be able to enhance the both patient and carer’s experience, and also embed new co-designed features to keep users motivated and supported.” said Clare
Find out more about OnTrack and the user-centred designs created by the Helix Centre.

In this blog our Managing Director for the Centre for Health Policy, Peter Howitt reflects on his experience attending the London Philanthropic Forum.