This blog post was written by Professor Kathryn Maitland, Professor of Paediatric Tropical Infectious Diseases at the Faculty of Medicine and Director of the Centre of African Research and Engagement at the Institute of Global Health Innovation, Imperial College London. She leads the SMAART Consortium (Severe Malaria Africa: A consortium for Research and Trials).
In much of sub-Saharan Africa (SSA), malaria remains a key cause of paediatric hospital admission, and makes a substantial contribution to under 5-year mortality, estimated at 600,000 annually.
Despite implementing currently effective, fast-acting artemisinin-based combination therapies, the multisite SMAART observational study has shown that inpatient mortality for paediatric severe malaria (excluding hyperparasitaemia with no additional severity features) remains unacceptably high at ~8%. The SMAART consortium was created in 2018 to translate recent advances in platform trial design to improve outcomes for severe childhood malaria across SSA.
SMAART is the only existing multi-site, multi-country collaboration conducting research in paediatric severe malaria on the continent.
SMAART-MAP, a multi-country adaptive platform trial (ISRCTN79071535) is simultaneously evaluating three adjunctive therapies in Phase II trials across SSA, addressing severe malaria complications (seizure prophylaxis, transfusion strategies and renal protection), with biomarker or clinical therapeutic efficacy endpoints based on putative mechanisms of action, to identify the most promising interventions to take forward into a large Phase III/IV mortality endpoint trial. The trial is being run in eight hospitals across six African countries (Ghana, Democratic Republic of Congo, Uganda, Kenya, Zambia and Mozambique).
The SMAART consortium is a multidisciplinary collaboration currently involving partners from SSA, Europe and Thailand with strong track records in delivering high impact guideline-changing treatment trials in paediatric severe malaria. SMAART’s ambition is to improve short and long-term outcomes for children with severe malaria in SSA by conducting better research studies faster, coordinating current and future research more productively, and hence enabling evidence-based continuous updates of disease definitions and treatment guidelines.
On International Women’s Day, we shine a spotlight on the incredible women at the Institute of Global Health Innovation (IGHI) who are shaping the future of healthcare worldwide. From pioneering research to innovative policy work, these leaders are tackling some of the most pressing global health challenges —making a real difference in in the UK and beyond.
Group photo of IGHI staff at the summer social.
In this blog, we celebrate their achievements and highlight how their expertise and dedication continue to inspire change. Read on to learn about some of these fantastic women at the IGHI and discover key examples of their work.
Professor Bryony Dean Franklin – Visiting Professor at IGHI
Professor Franklin is widely recognised as a research leader within patient safety, both nationally and internationally. She has specific expertise in evaluating technologies that aim to reduce medication errors in both primary and secondary care. She led a recent revision of the World Health Organization’s Medication Safety Curriculum Guide and has recently contributed to collaborative research and quality improvement studies in Brazil, India and Finland. As Co-Editor-in-Chief of the journal BMJ Quality and Safety she seeks to support and encourage others in publishing high-quality research and opinions that seek to improve patient care the world over.
Jennifer Bennett – Senior Postgraduate Administrator
Jennifer Bennett is a Senior Postgraduate Administrator for the PG Dip and MSc Digital Health Leadership (DHL) Programmes. She is responsible for the day-to-day administration of the programmes, supporting the students from recruitment to award and all the processes in between, working closely with faculty and teaching fellows to make sure the students get the best academic and pastoral support.
Jenny gained a new perspective on the student experience last year when she completed a L3 Team Leader qualification (CMI). She particularly enjoyed learning about leadership and communication models and evaluating how she could apply them to her work. This echoes the workplace assessments which the PG Dip students are doing, applying theory to practice. The PG students on the DHL programmes are all balancing work, study and personal or family commitments and Jenny has even greater empathy for students with looming deadlines! She is pleased to have achieved a Distinction. One of the projects she reflected on was the 2024 refurbishment of the office environment of 1070 at QEQM which has become a more inviting space for collaboration with colleagues.
Recently Jenny has introduced some processes to streamline the administration of benchmarking assessments and bulk uploading feedback to the VLE. She is also looking forward to contributing on further working parties to identify Imperial’s new VLE.
Melanie Leis – Director of Policy and Analysis
Melanie Leis is the Director of Policy and Analysis of the Centre for Health Policy, part of the IGHI. She leads the Centre’s development of analytics tools and policy outputs to support global decision-makers in fields such as patient safety, digital health and mental health.
Melanie leads our partnership with WHO’s Global Patient Safety Collaborative, which provides an opportunity to develop global and country-specific patient safety leadership support and resources. She also leads our collaboration with the charity Mental Health Innovations to deliver policy reports that highlight the key role that digital mental health services play in supporting the UK population. One of the projects she is most proud of is the collaboration with the charity Patient Safety Watch, through which IGHI produces reports on the national and global state of patient safety. The annual launch events of the reports bring together national and global patient safety leaders, including patients. These reports and events ensure that patient safety is at the top of system leaders’ agendas.
Jodie Chan – Public Involvement Officer, Helix Centre
Jodie Chan is a Public Involvement Officer at the IGHI’s Helix Centre, working on projects around safely involving women experiencing homelessness in research, understanding the mental health experiences and support needs of 10- to 13-year-olds, and analysing the impact of long waiting times on patients and the health system.
Jodie works across IGHI to support the meaningful involvement of patients, carers, and public members in research. Within her work, she has a strong focus on deepening and diversifying IGHI’s relationships with its local community and is passionate about supporting community-led research.
She is particularly proud of the relationships she has built with women at the Marylebone Project, a local women’s homelessness service, and of their ongoing work to make research safer and more psychologically informed.
Jessica Shields – Impact Officer, Helix Centre
Jessica Shields is an Impact Officer at the IGHI’s Helix Centre, working across the Centre to keep it running smoothly. Jess works on everything from supporting the scaling up of Helix projects and looking for funding opportunities to communications and coordinating Helix events. Jess also co-chairs the IGHI Wellbeing Working group, heading iniatives to improve workplace wellbeing at IGHI.
Jess is proud to support the Helix team to bring design to healthcare and being involved in the Wellbeing Working Group at IGHI. A particular highlight has been bringing the Helix team together over games and food for the Christmas All-Staff meeting and supporting team members to find funding for projects they’re passionate about.
Dr Jang Ah Kim – Lecturer at the Hamlyn Centre
Dr Jang Ah Kim is a Lecturer at the Hamlyn Centre for Robotic Surgery, Department of Mechanical Engineering. She is interested in researching multidisciplinary approaches to understanding and controlling the interactions between materials and their surrounding environments at the micro/nanoscale. By leveraging this knowledge, she aims to develop innovative and highly precise, minimally invasive strategies for biomedical sensing and robotics, addressing challenges unique to these scales.
The mini lab (micro-nano innovation lab) that Dr Kim leads is built on the belief that big breakthroughs start small. The lab focuses on micro and nano-scale engineering, exploring how light and other physical stimuli interact with materials to push the frontiers of biomedical sensing, soft robotics, and healthcare technologies. The name mini lab itself reflects this vision—written in lowercase to symbolise its commitment to micro/nano-scale research and precision-driven, minimally invasive healthcare solutions, where even the smallest changes can lead to transformative impact. Through this work, Dr Kim and her team strive to bridge fundamental science with real-world applications, advancing the next generation of biomedical engineering solutions.
Although newly established in September 2023, the mini lab has already embarked on exciting foundational research in manipulating micro/nanoparticles and bacterial swarms using light, as well as engineering shape-changing microrobots. These efforts aim to lay the groundwork for novel applications in personalised medicine, such as targeted drug delivery, cellular-level surgery, and local immunotherapy. In the long run, these highly targeted and efficient biomedical solutions could also contribute to addressing broader clinical challenges, including optimising therapeutic strategies and reducing unnecessary antibiotic use, ultimately supporting efforts to tackle antimicrobial resistance—all of which resonate with IGHI’s vision for advancing global healthcare innovation.
Dr Ana Cruz Ruiz — Project Manager, Hamlyn Centre
Dr Ana Cruz Ruiz is the Project Manager at the Hamlyn Centre for Robotic Surgery, where she coordinates centre-wide projects across various Technology Readiness Levels, ranging from basic research to medtech translation initiatives. In addition to this role, she leads the Hamlyn Centre’s Global Surgery working group, which focuses on how frontier technologies—such as AI, robotics, 3D printing, and the Internet of Things—can enhance surgical care in low- and middle-income countries.
One of her recent achievements includes organising the Global Surgery Forum at the Hamlyn Symposium 2024, where she co-moderated a panel with Dr Kee Park, Director of Policy & Advocacy at Harvard Medical School. The session, titled “Can Technology and Innovation Help Improve Health Equity?”, addressed the challenges faced by low- or middle-income countries in accessing safe, affordable surgical and anaesthesia care. The panel explored how technology is already helping to address some of these barriers, while also emphasising the need for further collaboration with the engineering community to create scalable solutions.
Ana is passionate about improving health equity in Honduras and in Latin America. Recently, she travelled there to meet with local surgeons, learn about regional needs, and explore ways to collaborate on making surgical care more accessible. She also contributes as a member of the Advisory Council for Honduras’ 2026 National Human Development Report, organised by the United Nations Development Programme.
Georgia Butterworth – Senior Strategy Advisor to Lord Darzi
Georgia Butterworth is a Senior Strategy Advisor to Lord Darzi, supporting the delivery of his wide-ranging portfolio across academic, policy and parliamentary priorities. In this role, she provides strategic advice and coordination across a diverse range of projects, from the Fleming Initiative to the NHS Independent Investigation. Her work is dynamic and varied, often requiring close collaboration with colleagues across the IGHI to ensure alignment across its centres.
One of the best things about my role is seeing the great achievements of the different centres in the IGHI and thinking about how we bring it all together for greatest impact. I find it really exciting to contribute to shaping the future of health and care through the IGHI, and inspiring to work alongside many exceptional women in this field.
Jessica Newberry Le Vay – Climate Change and Health Policy Fellow
Jessica Newberry Le Vayis a Climate Change and Health Policy Fellow in the Climate Cares Centre, working on the interconnections between climate change and mental health. Jess recently worked on the Connecting Climate Minds Global Research and Action Agenda, bringing together the perspectives of 960 experts across 100 countries to set out global priorities for climate change and mental health research and a vision for implementing and translating that research to action. Jess was also recently part of developing the People’s Petition, a global collective climate justice call submitted to the International Court of Justice in December 2024 that amplifies the testimonies of 18 witnesses from communities experiencing and responding to the worst impacts of the climate crisis, including impacts to physical and mental health.
Jess currently leads The Compass Project: Guiding minds and inspiring action through climate change education, working with young people and educators in schools and universities to ensure climate change education can equip and support young people with the resilience, knowledge, skills and agency to take climate action and live in an uncertain future.
Dr Emma Lawrance – Climate Cares Centre Lead
Dr Emma Lawrance is the Climate Cares Centre Lead and Mental Health Lead at the IGHI. Emma also leads the Wellcome-funded global initiative Connecting Climate Minds, which has involved over 1000 people across 100 countries to date. She holds an AXA Climate and Health Fellowship to more deeply understand the experiences of young people in the climate crisis in different cultures, what this means for their mental health and wellbeing, and to co-design and evaluate support that can build agency and resilience.
Emma is a recognised global leader in the emerging climate and mental health field, building awareness and capacity across sectors and countries to acknowledge and act for a climate of health and wellbeing. She is an author of key research and policy papers on the topic, including: the first global policy brief; leading reviews of the field as a whole, relevant interventions, and temperature and mental health; studies with young people in the UK, Caribbean and the US (under review), and the Global Research and Action Agenda for climate change and mental health. She has presented globally, for instance at the World Economic Forum, four UNFCCC COP conferences, the World Congress of Psychiatry, OECD and the European Commission and been featured in international media, including Die Zeit, Guardian, Al Jazeera, Sky News, BBC, Forbes, Reuters and others.
She believes in the power of community, and in connecting people and ideas to foster resilience to thrive in a changing world and to create a safer climate for our mental health.
Dr Laura-Maria Horga – Communications and Events Officer
Dr Laura-Maria Horga is a Health Communications and Events Officer at IGHI. She delivers communications and engagement projects across IGHI’s seven research centres of excellence, supporting the Institute’s mission to tackle global health challenges.
She is currently leading the organisation of IGHI’s annual in-person event, Demo Day, which helps staff learn more about the different workstreams at IGHI, connect with colleagues, foster collaborations, and celebrate the Institute’s achievements.
Dr Ivet Angelova has recently joined the MedTechOne programme at Imperial College London as a MedTech Specialist. Her journey into healthtech began with a PhD in Chemical Engineering, where she focused on developing genetically encoded biosensors for monitoring Botulinum Neurotoxins—a project that deepened her passion for turning scientific discovery into practical healthcare solutions.
Shaping the future of healthcare means not only driving research and innovation but also ensuring it reaches those who need it most. As part of MedTechOne, Ivet is currently working towards building a knowledge base that equips early career researchers (ECRs) with the tools to translate medtech discoveries into real-world impact. This resource is shaped by the needs and feedback of researchers across IGHI, the Hamlyn Centre and the wider Imperial community. Covering everything from regulations and quality standards to commercialisation and team building, this resource is designed to help bridge the gap between research and commercialisation. Additionally, she is co-leading the launch of the MedTech ECR Network at Imperial, creating a space for emerging medtech leaders to connect, collaborate, and thrive.
Ivet said “This International Women’s Day is a chance to celebrate the women driving healthcare forward, breaking barriers, and shaping a future where innovation is inclusive, impactful, and accessible to all. I am grateful to be part of a community filled with inspiring women whose work and determination continue to push the boundaries of what is possible in medtech and beyond.”
Cohort 7 Trainees – Julia Anderson (JA) Training Programme
Caitlin Murphy is as a JA Behavioural Science Trainee in the Fleming Initiative team. She is working in a patient / public facing project focusing on the use of antibiotics and encouraging individuals to finish a course of antibiotics if prescribed.
Arlette Albert is another JA Behavioural Science Trainee in the Fleming Initiative team. She is working part-time alongside Caitlin to develop her skills in qualitative research, behavioural science, patient engagement, and co-designing interventions.
Miranda Watson joined as the JA Trainee in Digital Health. She is working in the Patient Safety team to develop her skills in translating evidence into measurable interventions to improve patient safety in virtual care. She is involved in reviewing the literature, extracting data, and critically appraising available literature to identify safety indicators relevant to virtual consultations.
Our third blog post for the two-year anniversary of the invasion of Ukraine addresses the importance of prioritising better care for children with complex long-term health needs.
This is part of a series of blog posts sharing insights from our Ukraine Health Summit, hosted in partnership with the British Red Cross to further efforts in supporting the delivery and restoration of health services in Ukraine. This piece is written by Alexandra Shaw, Institute of Global Health Innovation, Imperial College London, with colleagues.
Ukraine Health Summit: attendees chatting
In Ukraine, many children continue to be cared for in institutions. Estimates vary widely and suggest that between 90,000-200,000 children reside in these institutions, and approximately 20,000-50,000 of them have disabilities.12
Children have a range of disabilities including congenital abnormalities of the nervous and cardiovascular systems, foetal alcohol spectrum disorders, genetic disorders and chromosomal abnormalities, visual impairments, cerebral palsy and epilepsy.3 Factors impacting institutionalisation include poor infrastructure for children with disabilities, including education and community-based therapy services. There is a lack of crucial services, including rehabilitation and palliative care, and support in the community, making caring for a child with complex health needs even more challenging. Social challenges also drive institutionalisation including poverty, social stigma and the lack of support means families are left isolated.3 An estimated 90% of children placed in institutions have parents or family but are placed in institutions because of the challenges of caring for them in the community. Other factors include the inability of parents to care for their children, neglect or substance abuse.2
Impact of institutionalisation
In 2019, the 74th UN General Assembly adopted the resolution on ‘Rights of the child’which urges that family and community-based care should be promoted over placement in institutions, and that children with disabilities should enjoy all human rights and fundamental freedoms on an equal basis with other children, including access to a family life.4 Children living in institutional environments can suffer significant harm including the impact on their quality of life, their ability to adapt to society, mental health and overall development.5 Facilities often fail to meet basic needs, address individual requirements and provide emotional and social stimulation.
Institutionalisation can lead to poor physical and mental health outcomes, stunting and a lack of development from inadequate nutrition, and infectious disease. Children who have been institutionalised can be left with difficulties processing and integrating sensory information, poor language development, damaging behaviours and significantly shortened life expectancy.6 Staff to child ratios are often inadequate, leading to inappropriate methods of restraint, and a lack of supervision means children are not provided with adequate sanitary care, or assistance with feeding.2
Reform and impact of war
Before the war, the government had adopted the National Strategy on Reform of the Institutional Care System (2017-2026), however there have been delays in implementation and children with disabilities have been excluded included in these reforms.7 The war has made the situation for children with complex long-term health needs even more desperate. Whilst children with more mild disabilities are being evacuated, many children have been moved from facilities in the east of Ukraine to inadequate facilities in the west. This had led to overcrowding, further reduced staff ratios, and a lack of medical records leaving staff looking after children with no background information about their condition and care needs.8
In some cases, children have been returned to their families without support or guidance to ensure the child’s health needs are adequately met.1The European Commission has provided 230 million in humanitarian aid to the Ukrainian government which brings an opportunity to ensure disabled children benefit from the assistance provided to Ukraine.9
Ukraine Health Summit: Dr Ulana Suprun
Moving forward
There is still progress to be made to improve care for children with complex health needs in Ukraine. A unified approach is required which clearly defines the responsibilities and powers of government authorities and local organisations to apply standards to protect children’s rights and care. Key recommendations include:
1. Reform for the provision of community based care
Change of policy and legislation, alongside political commitment, to prevent future institutionalisation and protect the rights of children, particularly those with disabilities.
Implement programmes to develop long-term family-based environments for children currently living in institutions.
Develop services to support children and families in the community including early intervention, social care support systems, family-based care, rehabilitation services, social services and paediatric palliative care.
Enable a holistic approach to care for children with complex health needs, including the role of education, sport, family and culture.
2. Paradigm and cultural change campaign
Launch a comprehensive and sustained campaign to enable a shift in attitudes and paradigms across all professions and the workforce.
Implement policy and a public campaign to encourage a societal shift in the way children with complex long-term health needs are viewed.
Enable the empowerment of families to advocate for their own children and specialist needs.
3. Development of health and social care workforce
Implement educational programmes to increase the size of the workforce in the areas of medical rehabilitation services, paediatric palliative care and social services.
Upskill professionals and expand access to continuing development for staff working across paediatric health and social care.
Develop capability in the community for family members, carers, social workers, rehabilitation staff, and other allied professionals such as speech and language therapists to support children in the community.
4. Strategic allocation of reconstruction funding
Develop a strategic plan to guide the allocation of reconstruction and support funding for children to be cared for outside of institutions.
Enable collaboration across different ministries which oversee education, social care and health to bring a more unified effort towards reducing the number of children living in institutions.
Prevent the reconstruction and rebuilding of institutions and instead invest in foster care, family and community-based services.
Rights of the child: resolution adopted by the General Assembly. 74th UN General Assembly; 2019: United Nations.
Slozanska H, Horishna N. Functioning of boarding schools negative impact on pupils. Social work and education. 2021;8:18-41.
Huseynli A. Implementation of deinstitutionalization of child care institutions in post-soviet countries: The case of Azerbaijan. Child Abuse Negl. 2018;76:160-72.
Rosenthal E, Kurylo H, Ciric Milovanovic D, Ahern L, Rodriguez P. Protection and safety of children and disabilities in the residential institutions of war-torn Ukraine: The UN Guidelines on Deinstitutionalization and the role of International Donors. International Journal of Disability and Social Justice. 2022;2(2).
Two years on from the invasion of Ukraine, we share a series of blog posts highlighting insights from our Ukraine Health Summit last year, hosted in partnership with the British Red Cross to reflect on and support the delivery and restoration of health services in Ukraine.
The second blog post focuses on the prioritisation of health care reform across the Ukraine health system for recovery and stable peace, and is written by Niki O’Brien, Institute of Global Health Innovation, Imperial College London, with colleagues.
[Ukrainian flag colours. Credits: Tina Hartung/Unsplash]
The war in Ukraine has caused substantial disruption to a health system that was already having to manage complex transitions.1
In 2014 the Ministry of Health of Ukraine initiated a national strategy to improve quality and access to care and sought to address longstanding challenges in strengthening primary health care (PHC), among other reforms.2 Since then, a guaranteed benefit package to reduce out-of-pocket payments was set up and enrolment with contracted PHC providers expanded to cover over 70% of the population as of 2020.
Since 2014, initial armed conflicts in the Donetsk and Luhansk regions have had implications on regional health services. However, the ongoing Russian invasion in 2022 has led to widespread disruption and destruction of infrastructure and resources across the country. Nationwide attacks on civilian infrastructure also target healthcare facilities, with over 1,500 damaged or destroyed as of 15 June 2023.3 The occupied territories have been hit particularly hard and face a severe shortage of health care workers (HCWs), medications, and supplies. For example, in the municipality of Melitopol, half of the doctors were forced to leave in the first months of the war.4 National and regional progress towards health policy ambitions has been drastically curtailed as resources have been reallocated to the immediate needs of the emergency response including frontline medical care.
Armed conflicts cause both direct and indirect morbidity and mortality with the latter occurring from both communicable and non-communicable diseases (NCDs). As expected, a rapid increase in infections has been reported, and the destruction of the Kakhovka Dam may further affect many thousands of local inhabitants while increasing the risk of the waterborne diseases.5 Moreover, cancers, oncology, and stroke in particularly can occur as a result of or be exacerbated by stress-mediated pathways.6 In Ukraine, cancer mortality was already high, however, recent research suggests that war-related delay in care of four months for five of the most prevalent cancers could lead to an excess of over 3,600 cancer deaths in the coming years.4
The war has also interrupted reform at the patient, health delivery and policy levels which had been initiated through disease-specific lenses in secondary and tertiary care pre-2022. For example, a significant proportion of Ukraine’s radiotherapy is based on Cobalt-60, rather than modern linear accelerators (LINACs) reflecting a wider need not just to increase basic modern technologies (CT, MR scanners etc) but also to upgrade existing hospital infrastructure.7 Volunteer and humanitarian help are essential but currently fulfil only some of the gaps, challenged further by lack of a nationwide coordination to address the needs of healthcare institutions.
[Ukraine Health Summit: woman in the audience speaking]
Measures to support Ukraine’s health system both now and in the early recovery period will need to focus on investment in HCWs and working with patient groups. For HCWs, examining and addressing the various push-pull factors, at a policy and systems level are required to support return. Pull factors for return include security and the potential to resume professional advancement and renumeration by re-establishing links between health service delivery and continuing education. Subject to budgetary constraints, the Ministry of Health could consider capitation-based payments and non-financial benefits to encourage relocation to resource-limited geographic areas or specialties.
Research in post-conflict settings highlights the value of indirect financial incentives (e.g., subsidised meals, childcare facilities, support for continuing education) and non-financial incentives (e.g., career development, improved healthcare facility resources and infrastructure).8 Digital learning platforms can further offer HCWs the opportunity to develop their knowledge by undertaking education and training remotely. There is also a need to invest in the PHC workforce (both physician and non-physician) together with substantial investment support and treat patients in the post-war period.
Ukraine is fortunate to have strong physician and patient organizations who can advocate for the needs of patients and communities. Advocating across disease areas and advising on where treatment can be sought, these organizations connect to patients and communities through social media while also working with high-level policymakers to drive change. When ProZorro, an electronic procurement system was launched in 2020 as part of reforms, 100% Life, one of the largest patient organizations in Ukraine used data from the system to fight corruption, with tangible benefits for the Ukrainian health system.9
After one year of war, in 2023 the organisation had collected $968,000 USD for humanitarian aid and provided 4,773,296 packages of medical goods.10 In 2024, the organisation and its partners has continued to support health service delivery by facilitating training and purchasing medical equipment.11 12Importantly, all individuals, organizations, and groups involved in delivering and receiving health care in Ukraine must come together to through a ground-up, community-led approach to realise a people-centred health system and drive people-centred reforms.
To be successful, efforts must be driven by patient, community, and population needs, led by government, and supported by providers and other stakeholders across the public and private sectors. As further atrocities are reported daily as the war in Ukraine rages on, there may be a reluctance to prioritise the planning of future health services. However, health, and therefore health care, is a prerequisite for recovery and stable peace.
References
1. Roborgh S, Coutts AP, Chellew P, Novykov V, Sullivan R. Conflict in Ukraine undermines an already challenged health system. Lancet. 2022 Apr 9;399(10333):1365-1367. Available at: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(22)00485-8/
2. WHO. Health financing reform in Ukraine: progress and future directions. World Health
Organization, 2022. Geneva, Switzerland. Available at: https://www.who.int/ukraine/publications/i/item/WHO-EURO-2022-5639-45404-64974
3. Міністерство охорони здоров’я України. За понад 15 місяців повномасштабної війни росія пошкодила або зруйнувала 1 554 об’єкти медзакладів. Міністерство охорони здоров’я України, 2023. Kyiv, Ukraine. Available at: https://moz.gov.ua/article/news/za-ponad-15-misjaciv-povnomasshtabnoi-vijni-rosija-poshkodila-abo-zrujnuvala-1-554-ob’ekti-medzakladiv-
4. Khanyk N, Hromovyk B, Levytska O, Agh T, Wettermark B, Kardas P. The impact of the
war on maintenance of long-term therapies in Ukraine. Front Pharmacol. 2022;13:1024046. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9731218/
5. Pavlenko D, Pavlenko M, Pavlenko R. Advantages and limitations of teleophthalmology during the war in Ukraine. Graefes Arch Clin Exp Ophthalmol. 2023 Jun;261(6):1761-1763. Available at: https://link.springer.com/article/10.1007/s00417-022-05967-1
6. Jawad M, Hone T, Vamos EP, et al. Estimating indirect mortality impacts of armed conflict in civilian populations: panel regression analyses of 193 countries, 1990–2017. BMC Med, 2020; 18, 266. Available at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7487992/
7. Price P, Sullivan R, Zubarev M, Zelinskyi R. Radiotherapy in conflict: lessons from Ukraine. Lancet Oncol. 2022 Jul;23(7):845-847. Available at: https://www.sciencedirect.com/science/article/pii/S1470204522002984?via%3Dihub
8. Witter S, Tulloch O, Martineau T. Health workers’ incentives in post-conflict settings – a review of the literature and framework for research. ReBUILD RPC, 2012. London, United Kingdom. Available at: https://assets.publishing.service.gov.uk/media/57a08a7be5274a31e0000614/rebuild_hwi_lit_review.pdf
9. Hrytsenko, Y. Fight for life: how Ukraine is fixing medical procurement and serving patients better. Open Contracting Partnership, 2021. Available at: https://www.open-contracting.org/2021/02/22/fight-for-life-how-ukraine-is-fixing-medical-procurement-and-serving-patients-better/
10. 100% Life. 100% LIFE, A Year Of Courage. 100% Life, 2023. Available at: https://network.org.ua/en/100-life-a-year-of-courage/
11. 100% Life. With the USAID support, 100% Life covered all primary care physicians in Lviv the training. Available at: https://network.org.ua/en/with-the-usaid-support-100-life-covered-all-primary-care-physicians-in-lviv-the-training/
12. 100% Life. Japanese Ministry of Foreign Affairs funds purchase of equipment for Ukrainian hospitals. Available at: https://network.org.ua/en/japanese-ministry-of-foreign-affairs-funds-purchase-of-equipment-for-ukrainian-hospitals/
“No test is better than a bad test,” said Matt Hancock.
While we may tire of hearing slogans, the principle here is important.
Coronavirus antibody tests have been hailed as a game-changer for the pandemic and a way forward as we traverse these uncertain times. Antibodies are Y-shaped immune molecules produced by the body in response to an infection. They latch onto the offender – such as coronavirus – in a bid to thwart it. Your body keeps a record of the encounter, so that if it comes across the same pathogen in the future, it can quickly make more antibodies and launch an effective attack.
This is the basis for hedging bets on antibody testing for coronavirus. The idea is that the tests will flag people who have already had the infection and therefore might have protection from getting it again. And so these individuals could potentially be afforded greater flexibility than those vulnerable to the disease.
But it’s not that simple.
Despite being known for under a year, this is arguably one of the most studied viruses ever. Yet it’s still new, and there are many unknowns. Crucially, we don’t yet know whether having antibodies can prevent future infection. Or, even if they do, how long this immunity lasts – a month, a year, many years? These are all questions we must answer before a potentially dangerous over-reliance is placed on these tests.
With so many caveats, why are researchers at Imperial leading a major study of community antibody testing? While the tests’ power to indicate immunity is – as yet – far from clear, they have important uses beyond this. Rather than focussing on individuals, looking at widespread patterns at the population level could help to monitor the evolution of the epidemic, which will have important implications for easing of restrictions such as social distancing.
Antibodies vs antigens
Currently the most accurate way to look for antibodies is to perform a lab test called an ELISA, on a sample of blood. Antibodies are very selective about what they stick to – specific molecules called ‘antigens’ (in this case, bits of the coronavirus). In an ELISA, a blood sample is mixed with coronavirus antigens that are ‘glued’ onto a test surface. If antibodies are present in the sample, they stick to the antigens and this binding leads to a detectable signal, most commonly in the form of a colour change.
These lab-based tests are accurate and can tell us the exact amount of antibody in a sample, but they’re complicated to perform, and require expensive, specialised labs. This means it’s not feasible to roll out this kind of antibody testing at a national scale, when labs are already overburdened. That’s why Imperial’s REACT study is looking at the possibility of using home testing kits instead.
“The big advantage is that the home testing kits are really cheap to produce, easy to distribute and store at room temperature, and they completely bypass the lab,” says Barney Flower, Clinical Research Fellow at Imperial and member of the REACT study team. “The beauty is that you get participants to do the leg work and carry out the tests themselves, so it’s less of a capacity issue when resources are stretched.”
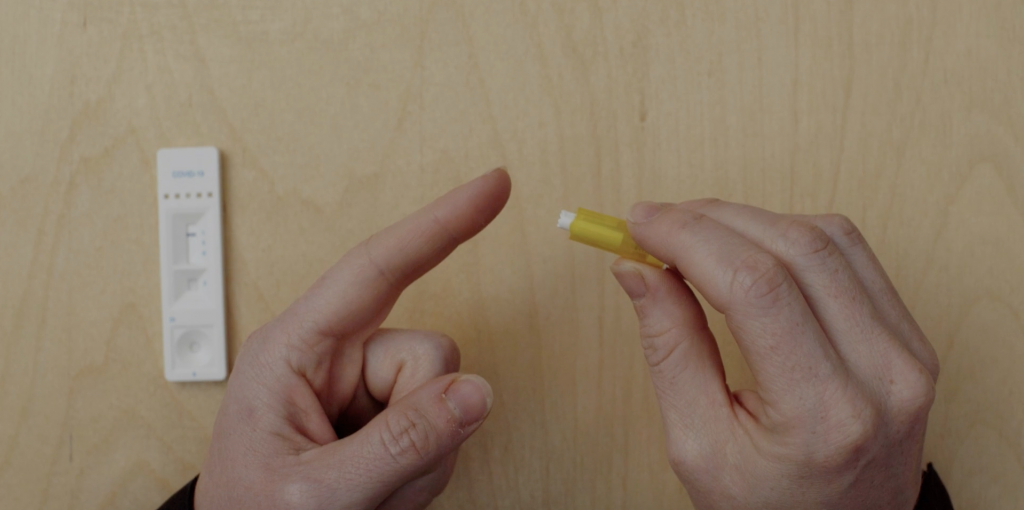
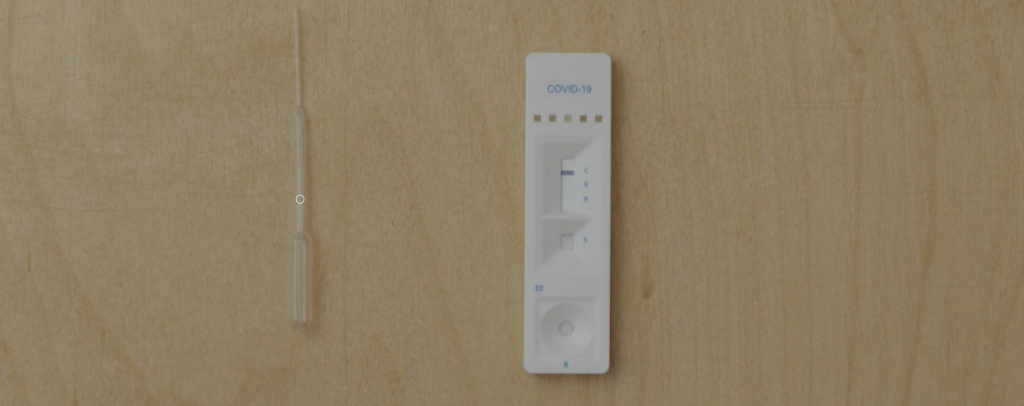
These home tests, called Lateral Flow Tests (LFTs), work in a similar way to ELISA, but everything is crammed into a small testing stick, which participants place a drop of blood onto. If antibodies are present, a signal will show up in a window on the testing stick, usually a coloured line.
The antibody testing kits display coloured lines depending on the result
A flooded market
By May of this year, already more than 200 of these LFTs had reached the market. However, there was no guarantee of their accuracy.
“The tests have been validated for use in laboratories, but in general their performance has been tested in small numbers of individuals, often fewer than 50 patients,” Barney says. “And these were usually individuals who were in hospital with COVID-19, so quite sick, and therefore more likely to have a strong immune response to the virus, producing lots of antibodies.”
This presents an issue, given that many people who have been infected with the coronavirus don’t have symptoms, and most don’t end up in hospital. So it’s critical to ensure that these tests work in this key group. And it’s also important to make sure that the tests perform well when they’re carried out by individuals themselves, not a trained technician – which is usually how they’re scrutinised in formal validation tests.
Antibody test results: true or false?
There are two main criteria that researchers use to assess how well an antibody test works. Its sensitivity is how well it picks up people who have been infected. If a test is 95% sensitive, for example, then out of 100 individuals who have had COVID-19, five will be wrongly identified as having not been previously infected (false negatives). Specificity, on the other hand, concerns the test’s ability to correctly identify those who were not infected. So if a test’s 99% specific, out of 100 people who haven’t had COVID-19, one will be wrongly identified as having been infected (a false positive).
In the UK, our regulator of medicines and medical devices (the MHRA), set out guidelines which stated that antibody tests need to be at least 98% sensitive to be able to guide decision-making in the clinic.
“The tests we’ve been looking at have been far below that,” Barney says. “So they’re no good at the individual level. But if we can find a test that’s really specific, we can make adjustments in our calculations and get a fairly accurate picture of the proportion of people who have antibodies at the population level.”
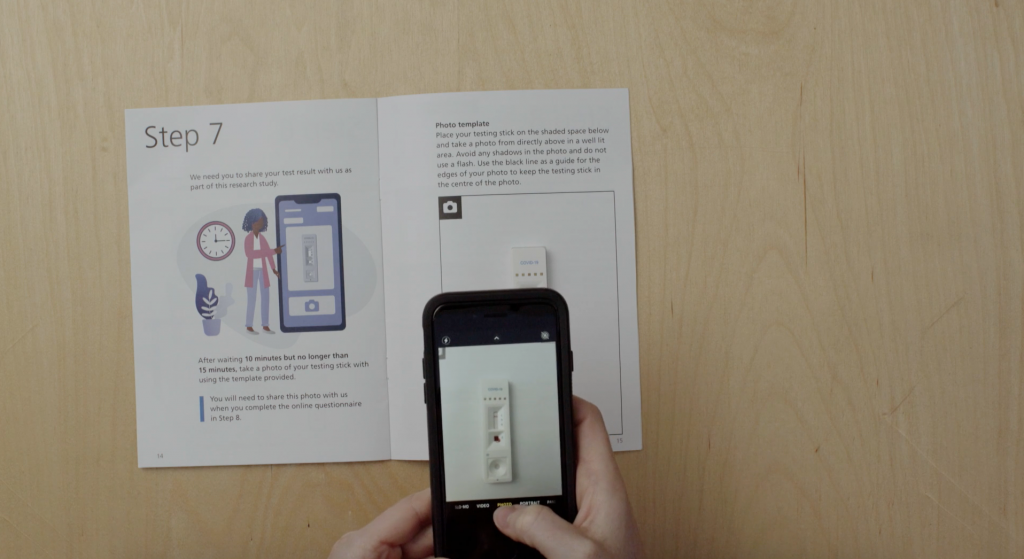
Study participants are asked to read the result of their test and submit a photograph so that researchers can review their interpretation
A testing conveyor belt
For the REACT programme, a team led by Professor Graham Cooke has been assessing a number of different commercially available tests, including the Wondfo test that the UK Government stockpiled early on in the epidemic. In the first phase, researchers carried out a small-scale study to test accuracy and usability (how well people can perform the test by themselves) on a group of around 270 healthy people, all NHS staff. Importantly, they’d all had a previous diagnosis of COVID-19 confirmed by a nose swab, but none of them had been hospitalised from the disease.
“The first test we tried out was throwing out negative results in four out of five participants – in a group who’d all had confirmed infection,” Barney says.
As well as testing the positive cases’ blood with the antibody kits, the researchers also performed an accurate lab ELISA to check if antibodies were detectable on the best test available. They found antibodies were present in more than 95% of cases.
They also tested the antibody kits on a batch of 500 blood samples taken from 2019 or earlier, i.e. preceding the pandemic and therefore COVID-19-free.
Together, this process is allowing the researchers to determine the tests’ sensitivity and specificity with a high degree of confidence.
“We’ve now developed a system where we can continually bring in new tests as they emerge, evaluate them on our bank of ‘known positive’ and ‘known negative’ samples, and if they look good we can test them in the clinic in more of a real-life scenario,” Barney says. “It’s like a lateral flow test conveyor belt.”
It’s how you use it
Another vital aspect of this work has been determining how usable these tests are by members of the public. Even if they perform well in controlled environments, they’re no good for use en masse if people can’t do them at home. A huge effort has been underway at Imperial, led by Prof Helen Ward, to involve and engage the public in this part of the project. Thousands of volunteers to date have given their time, offering valuable insight that’s not possible to gauge through lab testing alone.
While all of the LFTs work in the same way – placing a drop of blood onto a testing stick – there have been a number of issues with usability that this public involvement exercise has flagged up.
“This has been so important to highlight real issues with the tests,” Barney says. “One of the major things has been getting enough blood from the finger-prick, and successfully dropping this on the right part of the testing strip.”
At the start of the study, participants were provided with a plastic pipette to collect their blood after pricking their finger, which was then used to transfer a droplet of their blood onto the stick. But this soon proved a fiddly procedure, and now individuals are asked to place a drop of blood directly onto the test.
“We also found that health professionals tended to dive straight in and pay less attention to the instruction manual, and were therefore more likely to get it wrong!” Barney recounts. “Clear, simple instructions are so important!”
The leaflet to guide people through the at-home antibody test was developed with the public
Blood, spit, spots
While this research continues, the REACT team has narrowed down their hunt for the best home LFT. After analysing 11 different LFTs in the lab, they found the best tests could correctly identify individuals with coronavirus antibodies over 80% of the time, while also correctly ruling out those who don’t in more than 98% of tested individuals.
Based on these findings, the team selected and rolled out a finger-prick test to more than 100,000 people across England, who tested themselves at home in June and July. Covering all 315 local authorities to ensure a nationally-representative sample, this major study found that just under 6% of the population had antibodies to coronavirus and had therefore likely already had COVID-19. It also revealed that the virus hadn’t spread evenly across the country, disproportionally affecting key workers and Black, Asian and minority ethnic individuals.
Watch the video below for the study highlights:
Today we announced our findings of the world’s largest study on home coronavirus antibody testing. @imperialcollege researchers show that around 3.4 million people in England may have already had #COVID19, but that it hasn’t spread evenly across the country.
The team is continuing further testing of LFTs on a group of 5,000 key workers to gather more data. This particular piece of work is also investigating whether other methods could also be used for antibody testing, such as saliva samples or drops of blood dried on paper.
While this research can’t tell us anything about possible immunity levels, its offering is a greater understanding of how the epidemic is progressing, and who is at greatest risk from the infection.
“What this can help us understand is how many people have been exposed to the virus,” Barney says.
“Comparing these numbers to deaths and numbers admitted to hospital, in different populations and different parts of the country, will help plan for future outbreaks.
“However, it’s still important to say that we don’t know what these antibodies mean for individuals yet. Do they offer protection? And if so, for how long? The future of mass antibody testing rests on what we can learn from research like this.”
Type 2 Diabetes (T2D) is one of the greatest challenges currently facing the NHS, with growing levels of obesity contributing to a large increase in the numbers of people with the condition. The disease can lead to serious long-term health problems – including heart attack, stroke, kidney failure and sight loss – which have an enormous impact on the lives of patients and their families. And it is these complications that account for most of the healthcare activity and cost associated with T2D. (more…)
By IGHI guest blogger Chanice Henry, Editor, Pharma IQ & Pharma Logistics IQ
Similar to new Hollywood feature Rampage, a recent study has urged the life sciences industry not to underestimate the dangers that could hide within CRISPR Cas9.
Although the film has been criticised for wildly exaggerating the capabilities of the gene editing technique, it can be recognised for its effort to draw focus from the excitable buzz around CRISPR Cas9 towards the importance of considering the ethics and dangers associated with the tool.
A recent commentary piece also emphasised the importance of methodically debating the potential outcomes of CRISPR within the task of tackling Malaria.
Malaria is spread by the bite of female mosquitos holding the Plasmodium parasite. Plasmodium falciparum causes life threatening malaria.
Advances made so far
In the five years to 2015, 17 countries managed to eradicate malaria –including the likes of Senegal and Bolivia. In this period, mortality fell by 50% and incidences fell by 15% – preventing over 6 million deaths.
The World Health Organisation (WHO) recently launched “the world’s first malaria vaccine that has been shown to provide partial protection against malaria in young children.” After establishing efficacy in Phase 3 clinical trials a vaccine implementation programme is due to commence within this year’s immunization projects in Ghana, Kenya and Malawi.
A long way to go
Government spend on malaria prevention has seen a dramatic increase over the past decade. Although, experts note that around $6.5 billion of funding by 2020 will be key to hitting the WHO’s 2030 goal to wipe out malaria in 35 countries and shrink incidents and deaths by 90%.
Statistics claim that malaria still kills one child every two minutes.
Sub-Saharan Africa, as noted by Tanvi Nagpal, housed around 80% of the world’s malaria cases in 2016. “Their high infection rates are compounded by insufficient domestic budgets and struggling health systems.”Reports recently emerged stating of one in four blood banks in certain areas of Sub-Saharan Africa host supplies infected with malaria causing parasites.
Researchers are now turning to CRISPR Cas9 to stop the disease at the source of transmission – the mosquito.
What is CRISPR?
The genome-editing system based on CRISPR-Cas9 is becoming a valuable tool for different applications in biomedical research, drug discovery and human gene therapy by gene repair and gene disruption, gene disruption of viral sequences and programmable RNA targeting. The tool permanently manipulates gene expression by using programmable DNA nuclease and can remove faulty genes from a DNA sequence. (more…)
Even though drug development for Alzheimer’s Disease has a steep failure rate, the lessons learned from failed trials are of great benefit to future research.
Alzheimer’s is the most common form of dementia – the irreversible loss of memory and other cognitive functions which eventually makes daily tasks unmanageable.
However, the failure rates are high when it comes to creating new medical treatments to stop, slow or prevent Alzheimer’s. Between 2002 to 2012 there was a reported 99.6% failure rate within drug discovery for this condition.
Jeffrey Cummings notes that researchers have a duty to make sure that both the physical and financial efforts behind these failed trials are not in vain as they have a lot to contribute in the battle against Alzheimer’s.
Some key lessons from failed trials to incorporate into today’s R&D pipelines:
Animal testing has long played a key role in the development of drugs and the understanding of how diseases function. However, animal models also have critical translation issues when results are compared to human trials. (more…)
World Malaria Day is a good time to reflect on successes in the fight against malaria and the enormous challenges that still lie ahead. Malaria is a mosquito-transmitted parasitic disease, which causes illness ranging from severe flu-like symptoms to coma and death. Those at greatest risk are small children and pregnant women. It is an ancient enemy of mankind, and has exerted a powerful influence on our evolution. Malaria is a cunning foe, the parasites stay one step ahead of our immune systems allowing repeated infections to occur and they have a great capacity to develop resistance to antimalarial drugs.



 Jennifer Bennett is a Senior Postgraduate Administrator for the
Jennifer Bennett is a Senior Postgraduate Administrator for the 
 Jodie Chan is a Public Involvement Officer at the IGHI’s
Jodie Chan is a Public Involvement Officer at the IGHI’s  Jessica Shields is an Impact Officer at the IGHI’s
Jessica Shields is an Impact Officer at the IGHI’s 

 Georgia
Georgia



 Caitlin Murphy is as a
Caitlin Murphy is as a ![[Ukraine Health Summit: attendees chatting]](https://blogs-staging.imperial.ac.uk/ighi/files/2024/02/230425-owenbphoto-UkraineHealthSummit-028-1024x682.jpg)
![[Ukraine Health Summit: Dr Ulana Suprun]](https://blogs-staging.imperial.ac.uk/ighi/files/2024/02/230425-owenbphoto-UkraineHealthSummit-097-1024x682.jpg)



 In the five years to 2015, 17 countries managed to eradicate malaria –including the likes of Senegal and Bolivia. In this period, mortality fell by 50% and incidences fell by 15% – preventing over 6 million deaths.
In the five years to 2015, 17 countries managed to eradicate malaria –including the likes of Senegal and Bolivia. In this period, mortality fell by 50% and incidences fell by 15% – preventing over 6 million deaths. Even though drug development for Alzheimer’s Disease has a steep failure rate, the lessons learned from failed trials are of great benefit to future research.
Even though drug development for Alzheimer’s Disease has a steep failure rate, the lessons learned from failed trials are of great benefit to future research.