Protected: Turning lived experience into innovation: How Tamara Tortosa is building Qalyup
A resident doctor reviews a patient late in the day. The presence of an infection is uncertain. The guidelines are long and complex, and time is limited. The consultant wants a decision. The patient is expecting treatment.
Does the doctor prescribe antibiotics or not?
This is the reality of antimicrobial prescribing in hospitals. Decisions are often made under pressure, shaped not only by clinical evidence but by time constraints, hierarchy and patient expectations. These decisions matter. Every unnecessary or inappropriate prescription contributes, in small but cumulative ways, to a much larger global challenge: antimicrobial resistance (AMR).
AMR occurs when microbes such as bacteria, viruses, fungi and parasites no longer respond to the drugs used to treat them. It has been described as a “silent pandemic” because it builds gradually – in infections that take longer to treat, in extended hospital stays and in the slow narrowing of effective treatment options.
The scale of the challenge is stark. Global estimates suggest that AMR was associated with 4.95 million deaths in 2019.
Research led by Dr William Waldock, Clinical Research Fellow at our NIHR Northwest London Patient Safety Research Collaboration and supported by the Fleming Initiative and published in Nature npj responds to this wider challenge by exploring how antimicrobial resistance can be better measured across healthcare systems and addressed in clinical decision-making.
AMR is not just a scientific challenge; it is also behavioural and systemic. The knowledge needed to prescribe antibiotics correctly already exists in clinical guidance, alongside diagnostic information. Yet across hospitals and community care settings, this guidance can be difficult to use, inconsistently applied or overridden altogether.
In Dr Waldock’s two recent studies, the researchers set out to address this challenge from two complementary angles: how antimicrobial resistance is measured within healthcare systems and how clinicians can be better supported to make prescribing decisions in real time.
If AMR is such a significant global threat, why is it so difficult to control? Part of the answer lies in how it is measured.
Traditionally, AMR has been tracked through surveillance data – monitoring which bacteria are resistant to which drugs and where those patterns are emerging. While this provides an important picture, it does not always capture how resistance is experienced within healthcare institutions.
In the first study – Development of the antimicrobial resistance burden score through a modified eDelphi – the researchers highlight this gap and propose a new approach.
The study shows that relying on isolated indicators can be misleading. A hospital with high antibiotic use may still be practising strong stewardship, while another with lower reported resistance rates may reflect limited diagnostic capacity or incomplete reporting.
The AMR Burden Score brings these different measures together into one structured view, combining resistance patterns, prescribing practices and clinical outcomes. This allows healthcare organisations to better understand their AMR burden and assess whether interventions are making a meaningful difference over time.
In doing so, it provides a more integrated and interpretable picture of AMR within healthcare systems, allowing patterns to be tracked over time and the impact of interventions to be more clearly assessed.
If measuring AMR is one part of the challenge, the other lies in how prescribing decisions are made.
Antibiotic prescribing is rarely straightforward. Clinicians often need to make decisions quickly, sometimes with incomplete information, balancing the risks of under-treating infection against those of unnecessary antibiotic use. While guidelines exist to support these decisions, they are not always easy to apply in busy clinical environments.
The research highlights how this complexity plays out in everyday care, where time pressure, workflow design and differences in clinical judgement all influence how guidance is applied.
As Dr Waldock explains:
“In-hospital antimicrobial prescribing is frequently driven by the urgency of a deteriorating patient. While diagnostics are vital, clinical reality often demands pre-emptive intervention before full data is available. Junior doctors may occasionally have senior guidance, but more often, they must navigate these high-stakes initial prescriptions alone. In such moments, objective and accessible resources to guide the first response are invaluable.”
In this context, prescribing decisions are not made in isolation. They are shaped by interactions between clinicians, patient expectations and wider system pressures. This can create situations where decisions that seem appropriate for one patient in the moment may conflict with longer-term public health interests.
As Dr Waldock puts it:
“This reflects what economists call the ‘tragedy of the commons’ – where individual decisions, whether driven by clinical caution, patient expectation or organisational pressure, can work against the long-term interests of the wider population.”
This helps explain why improving antimicrobial use is not simply a matter of producing better guidance. The challenge is not only what clinicians should do but also how they are supported to make decisions in complex clinical environments.
It is this gap between knowledge and its application that the second study seeks to address.
If AMR is shaped by everyday prescribing decisions, the next challenge is how those decisions can be better supported.
In the second study – Enhancing quality of antimicrobial prescribing through ‘Ask Eolas’ (language model): a user-testing and simulation evaluation – the researchers explored how AI can support prescribing decisions in clinical settings.
Ask Eolas is an AI-supported clinical decision tool designed to help clinicians access the right antimicrobial guidance more quickly and accurately. The tool retrieves and summarises reliable clinical guidance while providing clear links back to source material, allowing clinicians to verify its recommendations.
On the value of Ask Eolas in clinical settings, Dr Waldock notes:
“Ask Eolas appears to make the prescribing process much safer and more reliable. Unlike previous tools that could feel like a ‘black box’, this technology is transparent about why it is making a suggestion. This gives clinicians more peace of mind and makes their daily workflow feel much smoother.”
In a structured simulation study, Ask Eolas outperformed both traditional PDF guidelines and existing digital tools. Participants using the system achieved fully accurate prescribing decisions across the study scenarios.
Clinicians also reported higher confidence and lower cognitive workload when using the tool, describing it as clearer and easier to use than traditional guidance formats.
This highlights that improving antimicrobial use is not only about providing the right information, but about presenting it in a way that can be used effectively under pressure.
While these findings are based on a controlled simulation, they provide early evidence that carefully designed AI tools could support safer and more consistent prescribing in clinical settings.

Together, these two studies outline a more connected approach to antimicrobial stewardship, where better data and better decision-making reinforce one another.
The AMR Burden Score provides a more complete view of how AMR is developing within healthcare systems, while Ask Eolas supports clinicians to make more accurate, evidence-based prescribing decisions in real time.
This reflects a wider transformation in healthcare. Rather than relying solely on static guidance and retrospective review, there is growing interest in more responsive systems that can support clinical decisions as they are made.
Looking ahead, Dr Waldock points to a move towards a more “agentic” hospital:
“The agentic hospital is a shift from doctors using tools to doctors leading a team of ‘agents’ in the delivery of healthcare. Instead of a computer just holding your medical records, it’s now an ‘agent’ that supports your care: spotting risks before they happen, coordinating your tests instantly and handling the paperwork so your doctor can spend their time focusing entirely on you.”
There is still more to do. Both studies highlight the need for further validation, real-world testing and continued collaboration across healthcare systems. They also demonstrate what is possible when research is grounded in real clinical challenges and designed with end users in mind – central to the Fleming Initiative’s work in harnessing technology for real-world impact.
AMR may be shaped by decisions made every day. Strengthening how those decisions are supported in clinical settings will be central to any meaningful response.
The Institute of Global Health Innovation (IGHI) at Imperial College London will showcase its work in digital health, leadership and policy at Digital Health Rewired 2026. The event brings together digital health leaders, innovators and policymakers from across the UK.

Taking place on 24–25 March at the NEC Birmingham, Rewired will bring together experts from across healthcare, technology and research to explore how digital innovation is transforming health systems. Across the two-day programme, IGHI researchers, educators and partners will take part in keynote conversations and panel discussions exploring how data, artificial intelligence and research-led leadership are shaping the future of healthcare.
Attendees will also be able to connect with the IGHI team during the event and learn more about how the Institute’s research, policy expertise and education programmes are supporting the next generation of digital health leaders.
On day two of the conference, IGHI will host the MSc Digital Health Leadership Dissertation Panel, highlighting how research undertaken by NHS professionals through IGHI’s Digital Health Leadership Programme is driving improvements across the health service.
Since the programme launched in 2018, around 160 NHS digital leaders have undertaken research projects addressing complex challenges within their organisations. Many of these studies have strengthened the evidence base for innovation, supported better decision-making and delivered tangible improvements in care.
Kenny Oniti, Senior Teaching Fellow at IGHI and chair of the session, said:
“The Dissertation of Practice projects enable students to tackle real-world challenges, anchoring their learning to organisational priorities and evidence-based practice to create measurable value for the NHS.”
During the session, recent graduates from the MSc in Digital Health Leadership: Vicky Kong, Antonia Brown and Adrian Jonas will share insights from their research, including the challenges they encountered, the lessons they learned and the impact their work is having within the communities they serve.
On day one of Rewired, Dr Hutan Ashrafian, Honorary Senior Research Fellow at IGHI, will join Professor Gillian Leng, President of the Royal Society of Medicine, for a keynote conversation examining the transformative role of artificial intelligence in healthcare.
A surgeon, entrepreneur and internationally recognised researcher, Dr Ashrafian is among the world’s most highly cited scientists and has worked at the forefront of translational clinical research, AI trials and health policy.
His recent research on the role AI can play in breast cancer screening has received significant media attention.
In this session, the speakers will explore AI as both a driver and product of health innovation. From real-world advances in mammography and surgical practice to questions of regulation, workforce development and risk, the discussion will examine how AI is reshaping clinical pathways, discovery and decision-making, and what responsible adoption will require at this critical moment for healthcare.
Also on day two, IGHI will present work from a collaboration with Mental Health Innovations (MHI) examining how digital tools can better support the mental health needs of younger populations.
The session, “Beyond the dashboard: designing digital care for minds, bodies, and real people,” will share emerging findings from research exploring the needs of children aged 13 and under and the opportunities for digital health solutions to address gaps in current services.
The session will also introduce a new digital platform designed specifically to support younger users. The work reflects a broader ambition to develop digital health tools that respond to the realities of patients’ lives and experiences.
Speaking ahead of the session, Dr Chris Agape Ajah, Policy Fellow in Digital Health at IGHI, said:
“This session will highlight IGHI’s unique approach to innovation, grounded in insights from people with lived experience and data. This is exemplified through our long-term partnership with MHI and our upcoming report on the mental health needs of children aged 13 and under. I look forward to sharing these insights with delegates and expanding opportunities for collaboration.”
Together, these sessions highlight how research, education and policy expertise can work together to accelerate the digital transformation of healthcare.
If you are attending Digital Health Rewired 2026, come and connect with the IGHI team at stand A45, join the conversations across the programme and discover how research, innovation and digital leadership are shaping the future of healthcare.
Explore the full Digital Health Rewired programme and register on the Rewired website.
Simrika Amatya is a Youth Advisor to the Compass Project, an initiative led by the Climate Cares Centre exploring how education can best empower young people to live, work, and thrive in a changing climate. Throughout 2025, the Compass Project conducted group discussions, co-design workshops, and a survey with students and educators – facilitated by and designed together with the project’s Youth and Educator Advisors. In this blog, Simrika reflects on her experience with the Compass Project.
This blog was written by IGHI Teaching Fellow, Julien le Jeune d’Allegeershecque. It features reflections on wellbeing, belonging and flexibility in online learning from Julien and Dunya Al‑Hayali, a MSc Health Policy student.
More and more students are opting for online postgraduate taught (PGT) programmes. It allows people from diverse cultural, linguistic and professional backgrounds to balance study with work and caring commitments. Although flexible and convenient, the online environment doesn’t have in-person contact and it can present unfamiliar institutional norms. This can affect students’ confidence, engagement and academic outcomes.
In a recent presentation for Imperial’s Students’ Voice initiative, chaired by Monica Tolocica from the Imperial Institute of Lifelong Learning, Dunya and I explored the challenges of online education. Dunya shared insights from her experience as a MSc Health Policy student. The online master’s programme is delivered by the Institute of Global Health Innovation.
We are delighted to welcome two new Centre co-directors – Professor Christoph Lindner to the Helix Centre and Professor Marisa Miraldo to the Centre for Health Policy.
Earlier this month, more than 60 students from the latest cohort of the Digital Health Leadership Programme (DHLP) came together in York to mark the beginning of their learning journey.
Over two days, students had the opportunity to connect with their peers, meet the academic team, and gain an understanding of what to expect from the year ahead. The forum included sessions from experts on leadership styles and reflective learning, the CliftonStrengths assessment, and time working within newly formed peer support groups. A highlight of the event was an immersive induction game, where students worked in teams to solve a series of puzzles as part of a simulated crisis in the NHS referral system. (more…)
In the Philippines, where typhoons and extreme heat are intensifying, young people are not only witnessing the climate crisis, but they are also living it. The research project Rising Faster Than the Sea Levels is working to understand and support the mental health and wellbeing of Filipino youth as they navigate the climate crisis.

The study is an example of co-developed research done with researchers including Dr John Aruta from De La Salle University, researchers at the Climate Cares Centre and codesigned by the Young Person Advisory Group (YPAG). Sophia Pahulayan, a recent graduate of Dr Aruta’s, is a project facilitator who helped to manage the project and cofacilitate the group discussions alongside young people, a vital linking point between the young cohort and the researchers. This was especially true due to Sophia’s previous research, passion for climate change work, and her ability to speak the local Bisaya dialect in a country with hundreds of dialects and local languages.
Sophia Pahulayana talks about connecting to young people for Rising Faster than the Sea Levels
Sophia recruited young people in the area to join the committee which was part of the decision-making process for the research materials and group discussion conversations. This helped to make the project more relevant to the experiences of young people when conducting semi-structured group discussions. This project helped to create spaces where young people can share their experiences of climate change and feel less alone. What makes this more natural free-flowing approach powerful and inclusive is its emphasis on solidarity and active listening. Sophia noted about the young people involved that: “they realised that they’re also basically the same. They may express it differently, but the core of the problem is the same.” The project tailors its methods to local contexts, using dialect and culturally resonant questions to foster trust and connection.

Sophia explained that the initial prompts were focused on big topics and concepts around climate change and mental health before YPAG realised that the better approach would be to focus on how local changes affected them and those they cared about. While young people may not always have the precise language for climate anxiety, they are deeply aware of how the climate has changed in their lifetimes. “They notice it has gotten different from when they were younger,” Sophia said, “they could still play outside during the summer, but now it’s not the same”. She also highlighted how they wanted the young people to make that connection between the climate crisis they’re seeing to the emotional struggles and the general anxiety they have when talking about the future.
Sophia Pahulayana talks about how Mental Health doesn’t exist in Filipino languages
For the young people, the project provides a space for validation and empowerment. As Sophia explains, their conversations are deeply intertwined with politics, as they are acutely aware of how government policy and corruption intensify climate catastrophes. They discuss painful memories like the mishandled billions in relief funds after Typhoon Yolanda which severely impacted their developmental years. The typhoon left survivors in their communities without adequate food, housing, or jobs and the corruption after made recovery even harder for the community. To finally voice these frustrations in a supportive environment is profoundly empowering. It transforms a sense of isolated helplessness into a shared realisation: “I’m not the only one thinking this way. I’m not the only one being concerned about this.” This awakening fosters a powerful sense of solidarity, making them feel less alone and more emboldened to empathise and get involved with climate action with their peers, a link which has been highlighted in a study published in Educational and Developmental Psychologist. The study says that “Filipinos who face a greater risk from climate consequences engage in actions that mitigate the climate crisis and prepare for future disasters.”

For Sophia personally, she describes the project as a source of hope and purpose. It allows her to connect with young people on a profound level, facilitating not just discussions but the birth of actionable ideas. Asked what she finds most rewarding about the project, Sophia explained that it is hearing participants say the sessions have given them hope and taught them things they never learned in school.

However, this hope is coupled with a driving urgency: “it gives me hope, but at the same time it makes me feel like there’s so much more that we could do”. While processing this emotional weight is crucial, Sophia is eager to take the project to the next level: moving from conversation to concrete action. The goal is to harness this newfound solidarity and sense of agency to help these passionate young people channel their feelings into tangible change within their communities, transforming hope into a resilient force for the future.

The plan is to host spaces like the group discussions where young people and researchers alike can combine the therapeutic benefits whilst also allowing connections with their peers. Young people already working to address the climate crisis need to be provided with a space to collaborate and bring their ideas to life. However, the space also needs to be one where young people can unpack what’s happened to them and deal with the trauma that was ever present when discussing climate disasters like Typhoon Yolanda. Spaces similar to climate cafes can be healthy places to decompress and provide emotional support to young people looking to act against future climate events in their community. Sophia does emphasise that whatever is created must be “tailored to our needs, to the needs of our community and our context.”
Now that the project team has completed the group discussions, they are working on designing interventions. On the 24 September they will be going to Cebu city in the Visayas region of the Philippines to present the preliminary results of the project. This should hopefully open the project to wider connections in the climate action space in the Philippines as a lot of the work takes place in the capital of Manila and few if any of the organisations in this climate crisis hotspot focus on mental health. The project has also just won $30,000 to expand their research in collaboration with John Aruta and Renzo Guinto and Duke University.
Sophia Pahulayana final takeaways from the Rising Faster than the Sea Level project
Rising Faster than the Sea Levels is a project led by Climate Cares Centre funded by AXA Global Research Fund
Further Reading:
Ten years after Haiyan: Building back better in the Philippines
2013 State of the Climate: Record-breaking Super Typhoon Haiyan
The Need for Mental Health Support for Environmental Defenders in the Philippines
Veronica’s Lived Experience story – Mental health impacts of climate change – Philippines
An agenda for climate change and mental health in the Philippines
Climate change and mental health in the Philippines Special Paper
Co-investigators: Dr Emma Lawrance, Dr John Jamir Benzon Aruta, Dr Ans Vercammen, Prof Fiona Charlson, Dr Chloe Watfern, Teaghan Hogg, Dr Sandeep Maharaj, Sophia Pahulayan, D, Georgia Monaghan, Court Kovac, Dr Daniella Watson
Affiliations: Imperial College London, UK; De La Salle University, Philippines; Curtin University, Australia; The University of Queensland, Australia; University of New South Wales, Australia; University of Canberra, Australia; The University of the West Indies, St. Augustine Campus, Ecomind, Australia
In partnership with the Jason Roberts Foundation, our team at Change Lab has been exploring how to better support Black men, when it comes to understanding prostate cancer and encouraging participation in early detection initiatives. This project was generously funded by the Bob Willis Fund and its work forms part of the LIMIT study which is contributing to wider efforts to make diagnostic research more accessible, inclusive, and responsive to the needs of communities often underrepresented in uptake of cancer testing.
The LIMIT Study tests a new MRI scan that can take place in the community and allows for prostate cancer to be detected in just 5-minutes.
Prostate cancer is the most common cancer in men in the UK. While significant progress has been made in improving how we detect it, early diagnosis remains a challenge, particularly for groups at higher risk. Approaches that use Magnetic Resonance Imaging (MRI) support early detection, such as those developed in trials like ReIMAGINE and Prostagram.
Black men face twice the risk of being diagnosed with and dying from prostate cancer compared to men of other ethnicities. In the UK, 1 in 4 Black men will develop prostate cancer, with 1 in 8 succumbing to the disease. In contrast, men of other ethnicities face a 1 in 8 lifetime risk and a 1 in 24 chance of mortality.
The ReImagine study also revealed that Black men were significantly less likely to respond to traditional GP-led screening invitations, with response rates only one-fifth that of other men. This gap highlights the urgent need for culturally tailored evidence-based engagement strategies.
Therefore, this project focused on partnership with a local Northwest London community organisation to co-create new approaches to improve uptake of prostate cancer testing in the Black community.
Change Lab formed a Patient and Public Involvement and Engagement (PPIE)_ group who helped shape the design of workshops that took place at the Jason Roberts Foundation (JRF) in Harsleden London. The JRF is a community organisation working at the intersection of sport and development, investing in local communities to change outcomes for the most marginalised and is recognised locally as a key community hub and have supported awareness of the importance of prostate cancer testing among their networks.
A core element of the project was the idea of the messenger effect – a behavioural science principle that suggests people are more likely to act on health information when it comes from someone they know or trust.
To explore this, the Change Lab team co-designed screening invitation materials with a group of men from different Black backgrounds who were over 45, including those with personal or family experience of prostate cancer. These materials aimed to make information about prostate cancer feel more accessible, relevant, and community-led. This took place through a series of workshops at the centre that resulted in one of the leaders from Jason Roberts Foundation, Head of Culture, Michael Adams synthesising these invites into community relevant materials such as a leaflet, video and WhatsApp message.
The collaboration with the Jason Roberts Foundation was a key part of this work as the community are experts by experience on how best to inform health improvement from the perspective of the Afro-Carribean community. The Foundation already had strong relationships with the local community and a shared interest in raising awareness of prostate cancer among underrepresented groups. As a result of this partnership, the Foundation have also began regular ‘health checks’ for community members where local people can come and have their blood pressure monitored at JRF.
Together, the Change Lab and JRF team:
This work was not about creating one-size-fits-all communications for the Black community. It was about working alongside communities to ensure that health messages reflect their realities, values, and needs as well as create materials that will resonate with improving uptake of cancer testing in the Black community.
The materials developed through this collaboration are due to be presented at a Prostate Cancer UK Roundtable. We hope that these insights will help shape the design of future studies, including the new £42 million national prostate cancer screening pilot.
The project also contributed to broader outreach work, including a segment aired on Sky Sports’ Blue for Bob Day 2024, in a cricket match between England and the West Indies, developed with input from the PPIE group and filmed at the Jason Roberts Foundation. These opportunities help raise awareness and ensure that conversations about health are happening in more places, with more people.
At Change Lab, we continue to reflect on how research can be more inclusive and responsive. Our work with the Jason Roberts Foundation is just one example of how university-community partnerships can help shape more equitable approaches to health.
By listening to and learning from those with lived experience, we aim to support research that not only improves outcomes but also builds trust and relevance across underrepresented communities.
This blog was co-authored by Helix Centre designers Sophie Horrocks and Tori Simpson.
From care pathways to medical products, healthcare can (and must) be designed to minimise waste, reduce emissions, and protect planetary health. This is not a distant vision, but an urgent necessity. As the world’s leading designers gather for the World Design Congress themed Design for Planet, here at the Helix Centre, we are exploring what it will take to make this ambition a reality, and the role human-centred design in healthcare can play in achieving it.
The connection between climate change and human health is increasingly clear. More frequent and severe heatwaves, floods, droughts, and storms directly harm health through injuries, heat stress, and other acute impacts. These events also indirectly affect communities by altering the spread of infectious diseases, driving food and water insecurity, damaging infrastructure, and deepening existing inequities. Together, they contribute to excess deaths and worsening physical and mental health outcomes (Haines et al., 2006; The Lancet, 2024).
Healthcare is also part of the problem. Globally, health systems produce around 5% of national CO₂ emissions in OECD countries (Pichler et al., 2019). In the UK, the sector accounts for 4–5% of total emissions, with the NHS in England responsible for about 40% of the public sector’s footprint (British Medical Association, 2024). At the same time, the climate crisis threatens the resilience of healthcare itself, with extreme weather disrupting services and rising health burdens straining already stretched systems.
These twin pressures highlight the urgent need for sustainable healthcare. By this, we mean the provision of health services in a way that meets the needs of today’s populations without damaging the health (or the ability to meet the healthcare needs) of people separated from us by time, geography, or socioeconomic status.
The challenge is significant, but it also highlights healthcare’s huge potential to drive change. Designing sustainable healthcare involves navigating trade-offs, such as balancing sterility requirements with reducing the footprint of medical equipment, while also seizing “win-wins” that benefit health, the environment, and even social and economic wellbeing.
At the Helix Centre (and Imperial College London’s Institute of Global Health Innovation more broadly) we’re exploring this challenge through six “wicked problems” at the crossroads of healthcare and sustainability. We have mapped these onto a matrix with the following axes, and for each, we share how we define the issue, present a case study of inspiring work in the field, and highlight sessions we plan to attend at the World Design Congress to deepen our understanding.
Through this article, we aim to open a conversation on how designers and other practitioners working in healthcare delivery (ourselves included) can integrate sustainability challenges into the heart of their work. If these themes resonate with you, we’d love to hear your ideas and examples and explore together how we can create healthcare systems that protect both people and the planet – get in touch with us at climate@helixcentre.com.

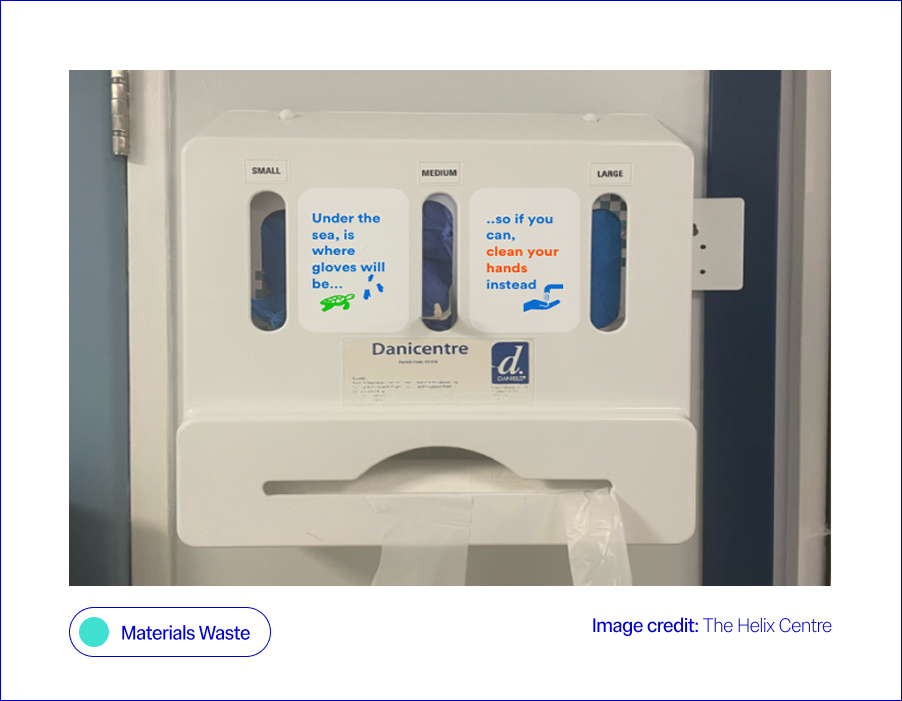
Every year, NHS England providers produce 156,000 tonnes of clinical waste. Tackling this could unlock major wins for both the environment and patient care. However, the answer isn’t simply reusing equipment. In healthcare, there is a complex trade-off between maintaining sterility requirements and limiting the environmental impact of medical equipment, particularly given that many essential items such as syringes and personal protective equipment (PPE) are single-use (Nicolet et al., 2022). Sterilising these single-use items for reuse can often be as carbon-intensive as replacing them after each use.
At Helix, we worked with a large NHS provider to test a behavioural “nudge” (a small design change that makes the sustainable choice easier without restricting options), aimed at improving hand hygiene practices and reducing the over-reliance on gloves. On hospital wards, glove use had become the default during the pandemic, often replacing standard hand hygiene practices like washing hands or using alcohol gel. To help staff return to safer, less wasteful habits, we co-designed a sticker for glove dispenser boxes, reminding staff when gloves were really needed. This small prompt (our “green nudge”) led to an 11% increase in hand hygiene compliance, meaning staff cleaned their hands more often at the right times, usually by washing with soap and water or using alcohol gel, in line with official guidelines (Blair et al., 2024). Outside of Imperial, the DesignHOPES team has worked with NHS staff to co-design a reusable theatre cap, designed to replace the current single-use ones. This intervention not only reduces waste but has also allowed for the personalisation of clinicians’ theatre caps, creating further wins for patient safety and staff identification. The Design for Life programme outlines an agenda and six fundamental challenges for our healthcare system in developing and embedding a circular system for medtech products.
Waste not, want not: from waste to wonder – a conversation between Sophie Thomas, Paula Chin, Adam Fairweather, Jo Barnard and Yaseed Chaumoo

What is the issue?
Care pathways are major contributors to the healthcare system’s carbon footprint. Fewer hospital visits, simpler procedures, and reduced prescribing could deliver large savings (NHS England, 2021). In summary, implementing quality improvement across care pathways with sustainability in mind can be a win-win in terms of environmental impact and patient outcomes (Health Foundation, 2025). Many trusts within the NHS are already assessing services against the Centre for Sustainable Healthcare’s all-encompassing definition of sustainability, which considers environmental, social and financial impacts as the foundational pillars in achieving sustainable services (NHS England, 2025). Alongside care pathways, food and transport services are listed as focus areas for the NHS’s green transition, cited as services that, if delivered more sustainably, could have a high impact on the NHS’s carbon footprint, with the two mentioned services comprising 20% of the health service’s total emissions (World Health Organisation, 2025).
Within Imperial, Matthew Harris explores opportunities for bidirectional learning between the NHS and low-income countries, including the implementation of various “frugal innovations” that use fewer resources to deliver healthcare, without compromising patient safety or clinical outcomes (Brown et al., 2023). Further afield, the GIRFT programme at Exeter University is developing a toolkit to map current carbon emissions and predict their impact on sustainability, financial aspects or care, patient outcomes, and equity of access. Within the NHS, the world’s first zero-emissions ambulance is being trialled in the West Midlands, setting an example for how other trusts can roll out more sustainable transport fleets, with the potential for dramatic carbon savings, given the NHS fleet is the second largest in the country (NHS England, 2023).
From Lab to Launch: How design accelerates Global Impact – an unconference with Paul Rodgers, Pete Broadbent, Suraj Vadgama, and Edward Hobson
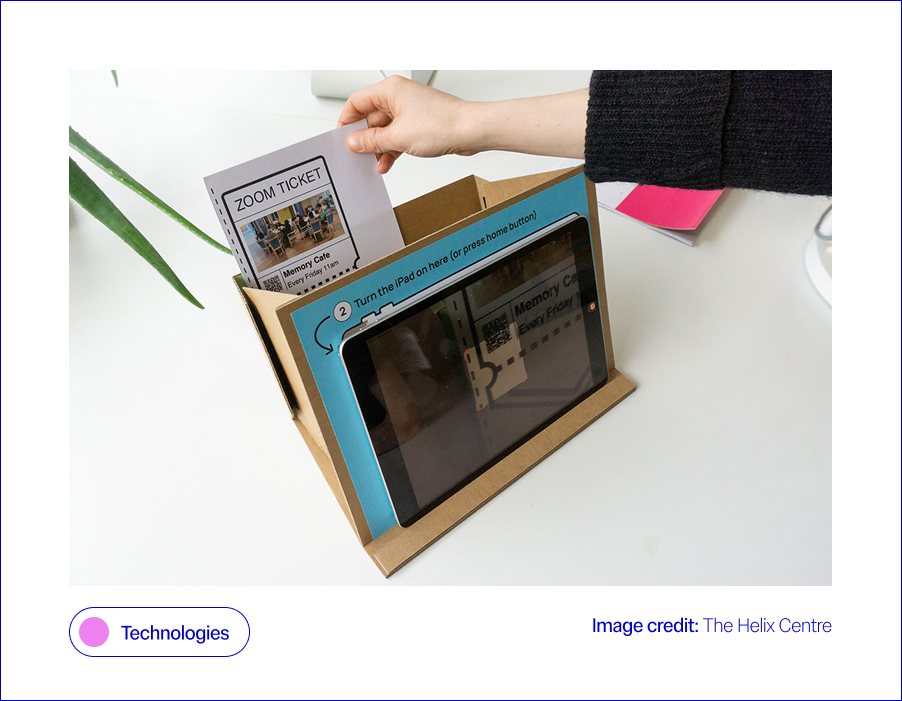
Technology, such as digital tools and remote monitoring to support care, is central to the NHS’s plan to cut emissions. Reduced transport costs, greater efficiency, and a focus on digital preventative care are all given as examples of how better use of technology could fast-track the NHS’s green transition (HSJ Information Ltd., 2025). However, with the intention to use AI systems to support many of these technologies discussed in the NHS’s recently released 10-year plan, it is important to consider the environmental impact of these technologies when implementing them (NHS England, 2025). It is estimated that globally, the data centres that power the technologies in question accounted for around 1.5% of global electricity consumption in 2024, with this consumption projected to grow by 15% per year (International Energy Agency, 2024). Similarly, a single data centre on average uses 300,000 gallons of water a day for cooling, enough electricity to power 100,000 homes (Ziegler, 2024). Finally, the move towards a more technologically enabled NHS also comes with a risk of digital exclusion for vulnerable parts of the population, which must be carefully considered within the transition (Health Innovation Network, 2023).
Previously, Helix collaborated with the London Office of Technology and Innovation (LOTI) to create a prototype system to support people with little experience of technology to participate in online meetings, mitigating the risk of digital exclusion as the healthcare system transitioned more to online engagement, following COVID-19, a decision that had a knock-on positive effect on carbon emissions (Rothwell et al., 2023). Within IGHI, Aws Almukhtar, supervised by Gaby Judah and Daniel Leff, is embarking on a project that will demonstrate surgical simulation as a novel research tool for testing and refining behavioural interventions designed to decrease carbon emissions from operating theatres. By testing interventions in simulated operating theatres, researchers can identify and refine the most impactful new approaches that improve sustainability and cut waste while maintaining quality before they ever reach a patient. Importantly, surgical simulation makes it possible to explore interventions, such as eco-labelling surgical instruments, that could not be tested feasibly in live operating theatres without prior supporting data.
Communities, AI, and Collective Impact – a panel discussion between Sevra Davis, Michael Bennett, Suma Balaram Schippers, Anne Asensio, Bharat Kapoor, Dr Ramit Debnath, Michele Morris, Jayden Ali, Mattie Yeta, and Dr Geke van Dijk
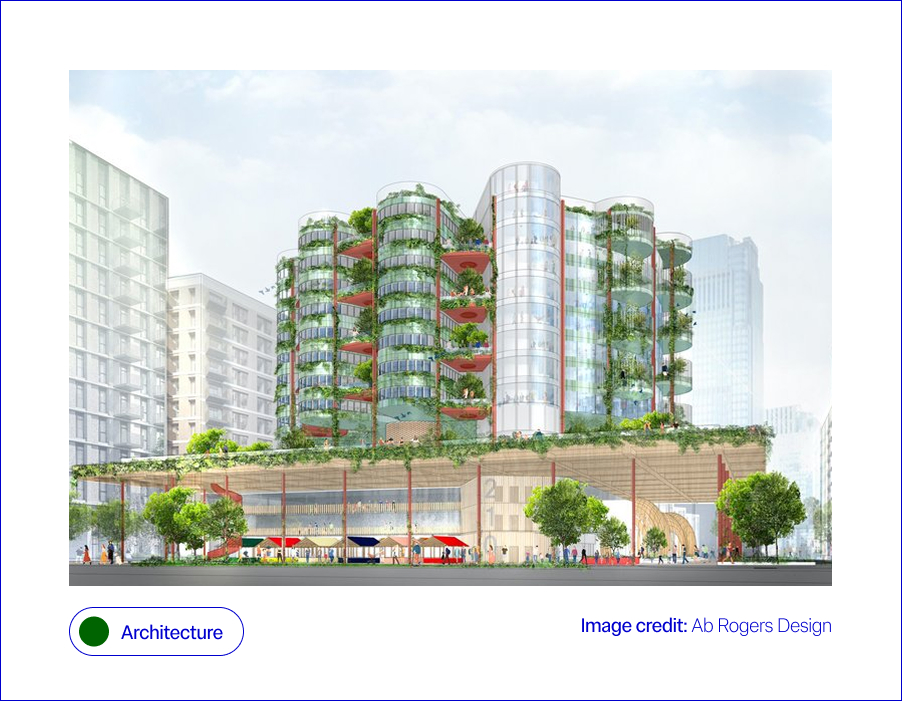
Hospitals are among the most carbon- and energy-intensive buildings, with 24/7 operations, complex equipment, and high heating and cooling demands. A 2024 systematic review highlights that hospitals contribute disproportionately to health sector emissions, with key drivers including energy use in buildings, embodied carbon in construction (the emissions tied to materials and construction), and waste streams (Public Health, 2024). Smarter building design and retrofits offer a clear path to reducing this impact. Alongside materials, “invisible” systems like ventilation or plumbing also affect sustainability performance and patient wellbeing. Climate change exacerbates these challenges, demanding that
hospital architecture becomes not only resilient to extreme weather, for example, floods and heatwaves, but also adaptive to future innovations. This means buildings must embrace digitally enabled architecture, where the physical fabric supports integration of new health technologies, automation, and data-driven energy systems (Design Council, 2021). In the context of architecture, sustainability is multi-layered, spanning bricks, wires, and human experience.
Responses span both future visions and practical action. Ab Rogers Design’s Living Systems reimagines hospitals as therapeutic spaces that integrate light, nature, and flexible layouts (RIBA, 2021). At a system level, the NHS Net Zero Building Standard (2023) is shifting net zero from exception to expectation. A powerful real-world example comes from Milton Keynes University Hospital, which re-roofed estate buildings and installed 2,586 solar panels. In 2021, these generated 853 MWh of electricity (around 8% of the hospital’s demand), cutting emissions, saving more than £225,000 annually, and improving patient comfort. The Trust plans to expand to 3,400+ panels, covering 15% of its needs (NHS England, 2021). Improving building resilience is also key: Loma Linda University’s hospital in California was designed to withstand seismic shocks, while UK trusts are retrofitting with double glazing and smart systems to reduce energy demand (Arup, 2023; BBC, 2023). Architectural consultancies like Buro Happold emphasise the need for adaptable hospitals that can withstand climate uncertainty while supporting patient wellbeing. Together, these examples show sustainability in healthcare estates is no longer aspirational; it is becoming standard practice for safer, greener patient care.
Design for Planet In Action: Fabrication, Futures, and Frontlines. Featuring: Samson Sahmland-Bowling, Peter Gitau, Alba Suárez Zapico, Charles Cambianica, Bethany Koby, Shajay Bhooshan
Building for the Future with Zoe Balmforth, Cameron Frayling, Hélène Chartier, Michael Pawlyn, Joanna Rowelle, Vanessa Miler-Fels
NHS England’s Greener NHS strategy identifies “models of care” as a priority, recognising that moving services from hospitals into communities can significantly reduce emissions while improving quality of and access to care (NHS Long Term Plan, 2019). This has been further emphasised by the recently released NHS ten-year plan, which sets out a vision for a “Neighbourhood Health Service”, which shifts care into local communities, to “reintegrate healthcare into the social fabric of places” (Department of Health and Social Care et al., 2025). Hospitals are resource-intensive, whereas community-based services allow greener, more localised alternatives through hub-and-spoke systems and preventative care.
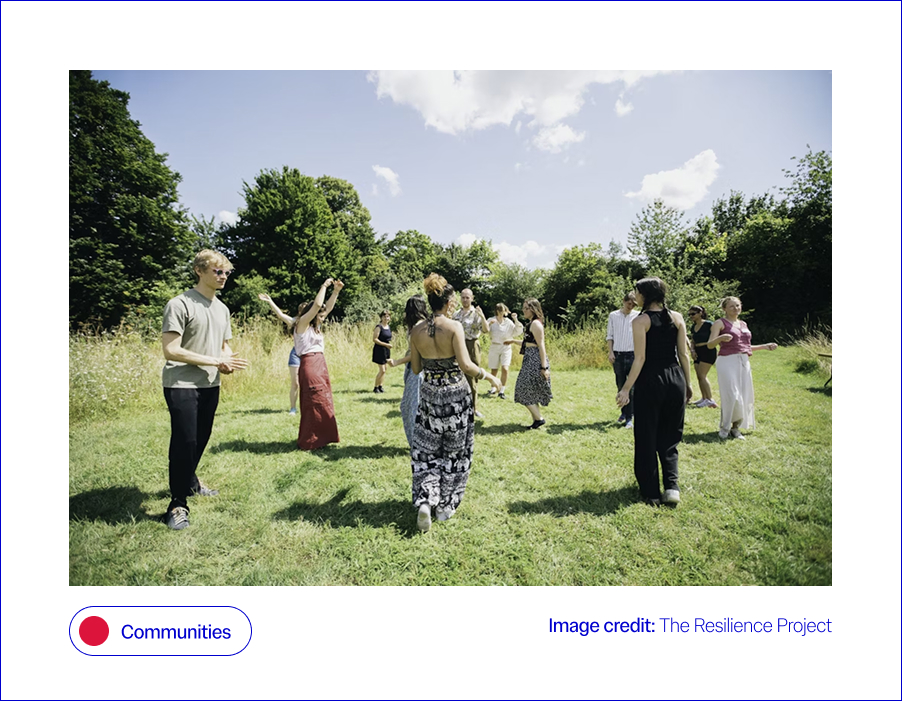
This shift is also vital for addressing the intertwined challenges of mental health and resilience in the face of climate change. Community-rooted care can provide both clinical and psychosocial support, enabling individuals and communities to adapt to climate-related stresses while easing pressure on hospitals. Community-based approaches, from preventative interventions to green social prescribing, demonstrate how models of care can reduce emissions while strengthening people’s physical and mental wellbeing (NHS England, 2021). Finally, any discussion of the built environment would be incomplete without noting the positive effects that access to nature and green space can have on health, mental wellbeing, and social connection, a powerful win-win where greener care spaces enhance both patient outcomes and climate resilience (Loveard, 2025). Ultimately, the challenge is not only to cut carbon but to reimagine care systems that also foster resilience, equity, and sustainability.
Innovative responses are emerging across different contexts. Within Imperial’s Institute of Global Health Innovation, the Climate Cares Centre is working with young people in the Philippines, Australia and the Caribbean to understand psychological responses to the climate crisis and co-design supportive interventions (Rising Faster than the Sea Levels). Climate Cares is also working to align climate change education and mental health support in schools and universities to support resilience building (the Compass Project). Climate Cares also works to connect and amplify existing initiatives around the world, such as ECO-MAMA, in Rwanda, which empowers women to safeguard mental health during climate stressors through an AI chatbot, and The Resilience Project in the UK, Europe and East Africa, which strengthens wellbeing through emotional regulation skills and social connection.
These programmes illustrate how initiatives can build resilience while broadening the ways in which care and wellbeing support are delivered. Building on this, research led by Matthew Harris has championed the role of community health worker models, drawing on international experience to strengthen local health delivery (Imperial College London, 2021). At the system level, the NHS has also expanded green social prescribing pilots, embedding nature-based activities into care pathways to support wellbeing and healthcare sustainability (NHS England, 2021). Together, these efforts sit within the broader framework of the NHS 10-Year Plan, which sets out a national roadmap for embedding greener, more personalised, and more resilient systems of care (NHS Long Term Plan, 2019).
Communities, AI, and Collective Impact featuring: Dr Geke van Dijk, Jayden Ali, Michael Bennett, Michèle Morris, Sevra Davis, Suma Balaram Schippers, Anne Asensio, Bharat Kapoor, Mattie Yeta, Dr Ramit Debnath

Sustainable healthcare requires action at every level, from national policy frameworks to the day-to-day choices of staff and patients. The climate crisis can feel like an added pressure for already stretched health systems, but there are clear “win–wins” to be found; just as insulating homes can cut energy bills and improve health whilst reducing emissions, similar opportunities exist in healthcare when policy and practice align. Top-down change is essential for embedding sustainability into governance, investment, and regulation, setting the conditions for lasting change. Simultaneously, bottom-up engagement is equally vital: sustainability can feel overwhelming or abstract for those working on the front line, so it matters how staff and communities understand and shape what is achievable in practice. Embedding resilience, therefore, requires not only policy and infrastructure but also a workforce that is equipped, supported, and motivated to act. Without this support, the resilience of the health workforce itself is at risk, with overwhelm and burnout threatening the very capacity needed to deliver sustainable care (Lawrence et al., 2024).
Behaviour change is a critical link between these levels; while many people recycle diligently at home, they may not apply the same habits at work or in public spaces such as hospitals. This underscores the importance of cultural as well as technical shifts, and the need to prioritise collective action, rather than an overemphasis on individual responsibility (Lawrance et al., 2022; van den Berg, 2015). Ultimately, progress depends on aligning ambitious policy with everyday behaviour change, supported by training and upskilling that empowers people at every level of the system (Michie et al., Behaviour Change Wheel).
Change is being driven from both the top down and the bottom up. At the policy level, the Health and Care Act 2022 made the NHS the first health system globally to embed statutory net zero and environmental duties into law, requiring NHS England, trusts, and integrated care boards to factor sustainability into their decisions (NHS England, 2022). This commitment is reinforced by the wider NHS Net Zero plan and efficiency-focused programmes such as Getting It Right First Time (GIRFT), which cut waste and emissions while improving care (GIRFT, 2024). At the organisational level, Green Plans provide a framework for trusts to set out three-year roadmaps towards more sustainable estates and services (NHS England, 2021).
Alongside this, bottom-up change is supported through training and workforce development: for example, the Climate Cares Centre at IGHI co-developed an Apolitical course, equipping policymakers with the knowledge and skills to address climate change and mental health simultaneously. Behavioural interventions are also crucial, helping staff to embed sustainable habits in clinical and operational settings; bridging the gap between what people already practise at home, like recycling, and what feels achievable in a healthcare context. To accelerate progress, policy must scale up these “win–wins” that make sustainable choices easier, so patients, staff, and organisations alike can help drive a greener future, through both everyday decisions and long-term strategies.
Designing the Economy We Need: Missions, Doughnuts, and Radical Collaboration with Mariana Mazzucato, Kate Raworth, Danny Sriskandarajah
The climate emergency is reshaping how we think about the way we provide healthcare. But this is also a design opportunity: to build systems that are not only safer and more effective, but also sustainable, resilient, and equitable. At Helix, we see our role as creating the conditions for this transformation: using human-centred design to tackle the toughest challenges at the crossroads of health and sustainability. The World Design Congress is a chance to learn, to share, and to build alliances with others who are equally committed to designing for the planet. Our contribution is to bring healthcare into this conversation, surfacing challenges, testing solutions, and creating space for collaboration. Beyond the Congress, we hope to serve as a bridge between designers and healthcare systems, so that bold ideas can become practical realities. By recognising these trade-offs and scaling the win–wins, we can design healthcare that is safer, greener, and more equitable, for both people and the planet.
With enormous thanks to Aws Almukhtar, Daniella Watson, Jessica Newberry Le Vay, Leila Shepherd, Matt Harrison, and Natalia Kurek, who have helped us shape our thinking in this space.
Arup (2023) Loma Linda University Health: Dennis and Carol Troesh Medical Campus. Available at: https://www.arup.com/projects/loma-linda-university-health-dennis-and-carol-troesh-medical-campus.
BBC News (2023) Milton Keynes Hospital installs solar panels to cut emissions. Available at: https://www.bbc.co.uk/news/articles/cz4dyj70dyvo.
Blair, C-J., McCrudden, C., Brazier, A., Huf, S., Gregory, A., O’Driscoll, F., Galletly, T., Leon-Villapalos, C., Brown, H., Clay, K., Maxwell, S., Anakwe, R. and Grailey, K. (2024) ‘A helping hand: Applying behavioural science and co-design methodology to improve hand hygiene compliance in the hospital setting’, PLOS ONE, 19(12), e0310768. doi:10.1371/journal.pone.0310768.
British Medical Association (2024) More support needed to help the NHS reach net zero. British Medical Association. Updated 28 June 2024. Available at: https://www.bma.org.uk/what-we-do/population-health/protecting-people-from-threats-to-health/more-support-needed-to-help-the-nhs-reach-net-zero
Brown, C., Bhatti, Y. and Harris, M. (2023) ‘Environmental sustainability in healthcare systems: role of frugal innovation’, BMJ, 383(8401), Article e076381. doi:10.1136/bmj-2023-076381.
Department of Health and Social Care, Prime Minister’s Office, 10 Downing Street, The Rt Hon Sir Keir Starmer KCB KC MP and The Rt Hon Wes Streeting MP (2025) Fit for the Future: 10 Year Health Plan for England. First published 3 July; updated 30 July 2025. Available at: https://www.england.nhs.uk/long-term-plan/
Design Council (2021) The Future of Health and Healthcare Design. London: Design Council. Available at: https://www.designcouncil.org.uk/fileadmin/uploads/dc/Documents/future-health-full_1.pdf.
GIRFT (2024) Getting It Right First Time: Net Zero and Sustainability. Available at: https://gettingitrightfirsttime.co.uk/cross_cutting_theme/net-zero-sustainability
Haines, A., Kovats, R.S., Campbell-Lendrum, D. and Corvalán, C. (2006) ‘Climate change and human health: Impacts, vulnerability and public health’, Public Health, 120(7), pp. 585–596. doi:10.1016/j.puhe.2006.01.002.
Health Foundation (2025) Why environmental sustainability must be at the heart of reform if the 10-year health plan is to help the NHS reap the benefits for patients, the health system and … [Blog]. Available at: https://www.health.org.uk/features-and-opinion/blogs/why-environmental-sustainability-must-be-part-of-the-10-year-health-plan
Health Innovation Network (2023) Bridging the Digital Divide in NHS Transformation: Ensuring Inclusivity and Equity [Blog]. Published 18 December 2023. Available at: https://healthinnovationnetwork.com/insight/bridging-the-digital-divide-in-nhs-transformation-ensuring-inclusivity-and-equity/
HSJ Information Ltd. (2025) Moving Towards Net Zero through Digital, HSJ Digital Awards [webpage]. Available at: https://digitalawards.hsj.co.uk/award-category/moving-towards-net-zero-through-digital
Imperial College London (2021) From Brazil to Westminster: Learning from a community health worker model. Available at: https://spiral.imperial.ac.uk/entities/publication/256305ad-73a4-4e7e-afa2-3c6af23369d2.
International Energy Agency (2025) Energy demand from AI. Paris: International Energy Agency. Available at: https://www.iea.org/reports/energy-and-ai/energy-demand-from-ai
Lawrence, W., et al. (2024) ‘Sustainable health systems and workforce resilience’, BMJ, 387, e081284. doi:10.1136/bmj-2024-081284.
Lawrance, E.L., Thompson, R., Newberry Le Vay, J., Page, L. and Jennings, N. (2022) ‘The Impact of Climate Change on Mental Health and Emotional Wellbeing: A Narrative Review of Current Evidence, and Its Implications’, International Review of Psychiatry, 34(5), pp. 443–498. doi:10.1080/09540261.2022.2128725.
Loveard, D. (2025) ‘Nature for Health: Making Green Space Work in Healthcare’, NHS Forest Blog, 23 June. Available at: https://nhsforest.org/blog/nature-for-health-resource-hub/
Michie, S., van Stralen, M.M. and West, R. (2011) ‘The Behaviour Change Wheel: A new method for characterising and designing behaviour change interventions’, Implementation Science, 6(42). doi:10.1186/1748-5908-6-42.
NHS England (2019) The NHS Long Term Plan. Available at: https://www.england.nhs.uk/long-term-plan/.
NHS England (2021) Green Plan Guidance for Trusts. Available at: https://www.england.nhs.uk/long-read/green-plan-guidance/.
NHS England (2023) Net Zero travel and transport strategy, in Net zero travel and transport strategy [Greener NHS]. Published 31 October 2023. Available at: https://www.england.nhs.uk/long-read/net-zero-travel-and-transport-strategy/#2-approach-and-methods
NHS England (2024) Greener NHS Strategy. Available at: https://www.england.nhs.uk/greenernhs/a-net-zero-nhs/areas-of-focus/.
NHS England (2025) Building on what we already do, in Understanding environmental sustainability [Greener AHP Hub]. Available at: https://www.england.nhs.uk/ahp/greener-ahp-hub/understanding-environmental-sustainability/building-on-what-we-already-do/
NHS England (2025) Fit for the Future: 10 Year Health Plan for England [webpage]. Published 3 July 2025. Available at: https://www.england.nhs.uk/long-term-plan/
Nicolet, J., Mueller, Y., Paruta, P., Boucher, J. and Senn, N. (2022) ‘What is the carbon footprint of primary care practices? A retrospective life-cycle analysis in Switzerland’, Environmental Health, 21:3. doi:10.1186/s12940-021-00814-y.
Pichler, P.-P., Jaccard, I., Weisz, U. and Weisz, H. (2019) ‘International comparison of health care carbon footprints’, Environmental Research Letters, 14(6). doi:10.1088/1748-9326/ab19e1.
Public Health (2024) ‘Hospitals’ contribution to health sector emissions: a systematic review’, Public Health, 232, pp. 74–86. doi:10.1016/j.puhe.2024.01.002.
RIBA (2021) Opportunities for health design research: Ab Rogers Living Systems. Available at: https://www.ribaj.com/intelligence/opportunities-health-design-research-wolfson-living-systems-ab-rogers
Romanello, M., Walawender, M., Hsu, S.-C., Moskeland, A., Palmeiro-Silva, Y., Scamman, D., Ali, Z., Ameli, N., Angelova, D., Ayeb-Karlsson, S., Basart, S., Beagley, J., Beggs, P. J., Blanco-Villafuerte, L., Cai, W., Callaghan, M., Campbell-Lendrum, D., Chambers, J. D., Chicmana-Zapata, V., … Costello, A. (2024) ‘The 2024 report of the Lancet Countdown on health and climate change: facing record-breaking threats from delayed action’, The Lancet, 404(10465), pp. 1847–1896. doi:10.1016/S0140-6736(24)01822-1.
Rothwell, E., Surtees, R., Allwood, D. and Gopfert, A. (2023) ‘Virtual appointments—embracing the opportunity to reduce carbon emissions mustn’t widen health inequalities’, BMJ, 381, Article p1169. doi:10.1136/bmj.p1169.
The Lancet (2024) ‘Editorial: Climate crisis and excess deaths’, The Lancet, 404(10419), p. 703. doi:10.1016/S0140-6736(24)01822-1.
van den Berg, M. (2015) ‘Health benefits of green spaces in the living environment’, Science of the Total Environment. Available at: [URL]
World Health Organisation (2025) How can health care facilities reduce their environmental footprint and contribute to more sustainable health systems?, Policy Brief 68. European Observatory on Health Systems and Policies. Published 8 July 2025. Available at: https://eurohealthobservatory.who.int/publications/i/how-can-health-care-facilities-reduce-their-environmental-footprint-and-contribute-to-more-sustainable-health-systems