Through our Master’s in Healthcare and Design, we aim to enable creative thinkers and change-makers to drive forward innovative, human-centred approaches to healthcare service delivery. If you want to lead innovation in healthcare systems, services and spaces, this is the course for you. To find out what it’s like to study with us, we caught up with Jeremy Chui, one of our alumni, who was awarded a distinction for this programme. Read on to explore some of the design projects that he worked on during his studies.
During our final year at Imperial College London, the three of us – Akhilesh, Jeannine and Hansa – came together with the vision to reduce healthcare inequity. Akhilesh was born and raised in London and is of Sri Lankan heritage. Hansa was born in India where she remained well into her teenage years and then immigrated to the UK with her family to finish high school, and has been in the UK for nearly a decade. Jeannine was born and brought up in Pakistan, where she is currently based, and spent four years at Imperial in the UK. So we have always known we wanted to break startup norms by starting off a business in a low-income country and then expanding that to the UK. We were born global. (more…)
Our MSc Health Policy Programme aims to equip students with the skills to critically evaluate existing and emerging health policies and nurture future health policymakers, both in the UK and internationally. This year, we have digitised and refreshed our course to provide students with a more flexible and engaged learning approach.
We’re pleased to have three students share their stories with us. They talk about their motivations to apply, enjoyable module experiences and how they use the knowledge they gained in their current work. Read their stories below and get a flavour of what it’s like to study with us.(more…)
Last year, our Institute launched a new fully online MSc Patient Safety Programme. Developed in partnership with Bayer Pharmaceuticals, the course aims to develop global leaders and changemakers in patient safety who can catalyse improvements and innovation in healthcare practice across the globe. As we open applications for its second year, we’re delighted to have a student from our first cohort, Charlotte Parsley, share her experience of the course with us.
“I have a clinical background in midwifery, specifically in patient safety and clinical governance. I chose to further my education with Imperial due to my strong interest in patient safety and Imperial’s academic reputation.”
The Imperial Breast Unit is an internationally renowned breast research centre and one of the largest breast units in the UK. The unit receives 150 new patients per week and around 400 to 450 new breast cancer cases are diagnosed each year. According to the National Cancer Patient Experience Survey (2011/2012), nine out of ten of the lowest-rated cancer patient experiences are at large London NHS Trusts.
Mr Daniel Leff, consultant breast surgeon at Imperial College Healthcare NHS Trust and programme lead for IGHI’s MSc Healthcare and Design, worked with postgraduate students from a range of healthcare and design backgrounds on the course using human-centred design to improve the patient experience at the Imperial Breast Unit. Read on as Mr Leff takes us through this innovative journey of redesign.
“In the MSc Healthcare and Design course, the education team introduces a healthcare design challenge to students. For this project, we embedded students in the breast unit to discover the potential challenges there with respect to patient experience. It was interesting that after the field trips our students identified a few major challenges.”
Challenges with the current design of the Imperial Breast Unit
“The waiting room experience was found to be poor. Every patient was lined up, facing each other, so that everybody could see each other. This created an anxious and stressful environment in the waiting room.
“The one-way patient flow also contributed to negative emotions among patients. Patients exited the counselling areas through the waiting room, which was the same route for them to enter the counselling areas. For those who received bad news, their facial expressions could be visibly distressed, and that made the waiting room experience more stressful for other patients. Worst still is that patients receiving bad news or a cancer diagnosis could feel very uncomfortable and self-conscious.”
What has been done so far?
“Students provided the course team with their very detailed patient feedback and qualitative research findings. They presented their findings to the external examiners, the Imperial charity, unit managers, and other key unit staff and brainstormed solutions.
“Working with the course team including leaders in design innovation at the Royal College of Art (Prof Ashley Hall and Anna Wojdecka), we then worked to further mature the initial ideas and then pitched the final design brief to the Imperial charity, and they decided to fund the final re-design.
“Based on the students’ findings, several changes have been implemented so far and there and there is more to come.”
Lucie’s Room
“They created ‘Lucie’s room’ which is a quiet place for patients behind the waiting room. Rather than going back through the waiting room, patients can exit the unit through a separate route via Lucie’s room, which provides a calming place for patients to process the information they received in their consultation and counselling sessions. There is a small kitchenette with a fridge and coffee making facilities in Lucie’s room for both the patients and staff to talk in a more relaxed, less clinical and more domestic and calming surrounding.
“The table in Lucie’s room is designed to split into two sections whereby two different conversations can be happening simultaneously. When Lucie’s room is used for meetings, the staff can connect the two pieces of the table, and everyone can sit around it, much like a boardroom configuration. The ideas behind Lucie’s room are therefore multifactorial, including escape route for patients with high expressed emotions, quiet calm space for nursing-patient discussions and modular design flexibility to facilitate staff multidisciplinary team meetings.”
New patient exit route through Lucie’s room
Dynamic art installation
“A prismatic dynamic art installation has been designed for the waiting room’s window. The idea behind the installation is that this acts as a distractor to alleviate anxiety. When the light hits the glass prisms, different ‘rainbows’ form on the waiting room. There is good evidence that positive distraction alleviates anxiety. Students also redesigned how patients are seated and where to put the reception desk to provide more space in the unit.”
Prismatic dynamic art installation for the waiting room at Imperial Breast Unit.
Hopes for a better patient experience
“The project team has almost finished the redesign. After its completion, researchers will follow up on this project and collect data to see if our work improves the unit environment and patient experience.”
A decade ago, Imperial medical student John Chetwood darted from his Varsity hockey match to try his hand at another competition, with a different prize at stake. It was the inaugural IGHI Health Innovation Prize, giving UK university students the opportunity to win cash towards their global health idea.
John was one of five finalists to face our panel of judges at the Dragon’s Den-style final, and took home the top prize of £2,000 towards his new diagnostic tool for an aggressive type of bile duct cancer.
As we launch this year’s event, a decade after it all began as the ‘Student Challenges Competition’, we caught up with some of our winners to find out their journeys since taking home the prize. If you want the chance to win £10,000 towards your global health idea, click here to find out more and apply now.
Spreading SMILE across the world
Kitty and Abellona, 2017 winners
“Our innovation, the SMILE (SMart-last mILE) vaccine cooling system, is the only last-mile solution that reduces human error and vaccination spoilage. It’s patented, low-tech (freeze-free) and fail-proof. SMILE can last for three to six days without power while monitoring and displaying the remaining cool-life of temperature-sensitive products, like vaccines.
“We have made a tremendous amount of progress since we won the IGHI competition. SMILE has been iterated, lab tested and field-proven. We conducted a successful field trial in remote villages in Madagascar at the end of 2019. We are entering the manufacturing and commercialisation stage. We are also working on an upgrade for a second version with extended features.
“SMILE’s help is not limited to developing countries. It will also help in biomedical research and cold-chain applications in the developed world. We are looking for trial partners in the UK and are keen to work with institutions to improve their work efficiency with SMILE.
“Winning IGHI has helped with running our IDEABATIC platform and helped raise awareness of the last-mile cold-chain challenges. After winning the competition, we won funding from the Expo 2020 Dubai, Royal Academy of Engineering and InnovateUK which also helped in this journey. We were also selected as finalists for the MIT-Solve global challenges.
“We encourage everyone who has a passion to solve important issues to take part. Make sure you tell people the story behind the innovation and share your passion with them. Good luck!”
Getting smart with parasitic worms
Laura and Kai, 2019 winners
Capta is a smart, low-cost tool to accurately and rapidly diagnose parasitic worm infections, which are responsible for soil-
Laura and Kai
transmitted helminth infections and diseases such as schistosomiasis. Compared to current labour-intensive testing, their handheld microscope uses machine learning and automatic imaging to analyse samples. The device also records data to provide real-time statistics on global disease burden. Team Capta hope that their tool will allow for faster diagnosis of these infections, and help target treatment to areas that need it the most.
“Winning the IGHI student challenge competition provided a huge opportunity for Capta. Shortly after the competition we expanded our team and used the funding to prototype the diagnostic tool. This was crucial to demonstrate to future partners and investors that we do have the capability and expertise to develop this tool. We have recently won a grant that will support our data collection in sub-Saharan Africa, and are excited to make progress following a break throughout lockdown.
“We couldn’t recommend the IGHI competition highly enough – it is a friendly pitching competition that provides a fantastic opportunity to network and meet fellow health-tech start-ups.”
Third Eye Intelligence: Buying time for people with organ failure
Sam Tukra, 2020 winner
Third Eye Intelligence is an artificial intelligence-driven platform that brings together a vast array of patient data to predicts their risk of organ failure, acting as an early warning system for doctors working in intensive care.
The platform design
“Ever since we won the Health Innovation Prize our development speed increased significantly. Following the award, we were able to hire bright engineers from Imperial College who were hungry to grow and implement their machine learning skills in a real clinical problem case. To wit, we completed our prototype of our early warning system for organ failure software to a presentable state. Using this new developed system we were able to present to 2 hospital partners whom we will be collaborating with for a clinical trial of our system in an intensive care unit.
“Currently, we are in the process of raising our seed round to fund this multi-centre trial to continue our development for market entry with product v1. Hence, the initial winnings from the health innovation prize really helped us to accelerate our growth not only from the technology development perspective but also from the commercial perspective. Additionally, the network effects from the pitching event, lead to attracting bright minds that joined our team and helped us grow Third Eye organically.
“My advice to student innovators would be, that Imperial is full of resources to accelerate their commercial journey that goes beyond R&D. Hence, just go out there and utilise all resources at your disposal, this includes competitions, events and more importantly people, that share your mission and can join your team to help you grow and reach the next stage.”
Could you be the next Health Innovation Prize winner?
Our annual student competition is open for applications, open to students at any UK university. Click here to find out more and apply for your chance to win £10,000 towards your global health idea.
Former winner Nate Macabuag presenting his project to the 2018 judging panel.
Almost half of all deaths in children under the age of five are linked to undernutrition. Most of these occur in the developing world. There is therefore an urgent need to address this pressing issue which costs the lives of millions of children every year. And as detailed below, the answer is not as simple as providing more food.
In a new Gut review, led by IGHI lecturer Dr Alex Thompson, scientists explore the role that technology could play in improving understanding, management and prevention of this complex condition, with a focus on low- and middle-income countries.
We caught up with Dr Thompson to find out more. (more…)
“We’re in this together.” One year ago, on 11th March 2020, the World Health Organization declared COVID-19 a global pandemic.
Back then, little over 100,000 cases had been reported globally. Today that number is 1,000 times greater and growing ceaselessly.
With a barely known virus rippling across the world, so too did fear and uncertainty spread as the WHO Director-General addressed all people and nations to make the declaration. Shifting the focus from COVID-19 to people and unity, Dr Tedros also sparked glimmers of optimism by emphasising that innovation and learning would be integral to saving lives and minimising the impact of the pandemic.
Innovation is the beating heart of IGHI, and we’re proud of our community that has joined this long and winding path of discovery in many different ways. A year on, our people reflect on their COVID-19 response journeys and impart the lessons they’ve learned along the way.
Read their stories below.
Tracking COVID-19 past and present – the REACT study
In April 2020 we launched the biggest and most comprehensive study of home coronavirus testing. With colleagues across the College, Imperial College Healthcare NHS Trust, and Ipsos MORI, the REACT programme has been testing hundreds of thousands of people across England every month to track infections past and present. Alongside understanding how many people are currently infected, REACT is identifying people who are most at risk of infection while offering a range of other important insights, such as antibody responses to vaccination. The programme has also worked closely with members of the public to ensure that the research is guided by people’s needs.
This work has been instrumental in the monitoring of England’s epidemic and offers robust, timely evidence on the evolving situation, which is continuing to shape the government’s response.
“One phrase has dominated Government pronouncements on the roadmap out of lockdown: ‘Data, not dates,’” said Professor Ara Darzi, REACT programme sponsor and co-director of IGHI. “And rightly so. The Covid crisis has caused terrible suffering, wrecking lives and livelihoods. But unless we understand it, we cannot defeat it.
“Among the most pressing questions over the last year have been how many people are currently infected with the virus, and how far has it spread through the population? REACT has been a key element of the effort to answer these questions, providing among the most accurate and up-to-date data on its progression across England.
“By regularly testing 160,000 randomly selected people every month, the study has played a vital role in informing the Government’s decision over when to impose lockdown and when to lift it.
“In doing so it has proved the central importance of accurate data gathering to control this and any future pandemic. We forget this lesson at our peril.”
Social distancing measures have helped keep the virus at bay, but not without cost. The loneliness and isolation that come with keeping people apart are negatively impacting people’s wellbeing, particularly so for those who depend on support from others in their everyday lives, such as people with dementia.
In response to this issue, our Helix Centre partnered with collaborators to develop a digital resource to help community groups create online networks as a way to maintain support and connection for people affected by dementia. Called Community Makers, the initiative is also building a toolkit of creative ideas for digital involvement, including how to reach people who may not have access to technology.
“Community Makers was a project that addressed a real-time need we saw in the people we were working with through our dementia research,” said Matt Harrison, senior designer at IGHI’s Helix Centre and project lead at Imperial. “People with dementia were some of the least able to adapt to lockdown measures and keep themselves isolated, yet very vulnerable to COVID.
“Collaborating daily with colleagues I have never met in person, at Alzheimer’s Society and University of Worcester, it has been inspiring to work with community groups across the country and see how they have adapted to using digital tools to support their members, and see how technology has evolved to match the need. However, the need is still not met, and there is much more to be done. The post-COVID world will be made up of the best of in-person and digital connections, and we are now seeking funding to help facilitate that change.”
Monitoring people’s changing attitudes and behaviours
Washing our hands regularly, taking public transport, avoiding meeting people outside of our household – many of the things we do affect our risk of COVID-19. Public health measures and campaigns have been designed to encourage people to behave in ways that reduce this risk, but how well are people sticking to them? And how are people’s attitudes in relation to the crisis changing over time?
Launched in March 2020 with YouGov, our ongoing COVID-19 health behaviour study is the largest of its kind, surveying thousands of people across the globe every month – half a million in total to date – to understand how citizens are responding to the pandemic. By making the findings freely available, and collaborating with a range of partners, our work is enabling decision-makers to tailor their response based on evidence.
“The stories that emerged, their common threads and their remarkable differences have helped many scientists, public health authorities, members of the press, government leaders and the public to come to grips with many of the driving forces behind the spread of COVID-19,” said Sarah P Jones, project co-creator and doctoral researcher at IGHI.
“When I look back across the year I’m struck by not the divisions sown between us, but by the overwhelming cooperation the world has generated.
“At the beginning of the pandemic I saw every new announcement as a rule, a constraint or a liberty taken away.
“But starting from the very first time YouGov returned our global survey results, I realised something incredible was happening in the world.
“Every hand washed, every mask worn, every metre of distance we placed between ourselves and others have been a gesture towards each other, a signal of respecting one another’s safety.
“I personally cannot wait to get back to hugging, to hearing stories in person and to caring for those I love who are still far away.
“But as we emerge from this cocoon the question on many peoples’ minds should not be “How can we get back to normal?” but rather “Is there anything we cannot accomplish together?”
Understanding the impact of the COVID-driven digital shift in primary care
Digital technologies have been poised to transform the delivery of health care for some time. When the pandemic hit, their promise was quickly put to the test as health systems were forced to shift much of their care from in-person to remote delivery.
Switching from face-to-face consultations to phone calls and video meetings has enabled services to continue while keeping both patients and healthcare staff safe. But what has been the impact for patients and professionals? Our international InSIGHT study has been working with global collaborators to explore this in primary care, using a survey to gather the perspectives of thousands of GPs across 20 countries.
“We were pleased to hear that GPs identified a range of benefits, including reducing COVID-19 transmission risks, guaranteeing access and continuity of care, greater efficiency, faster access to care, and improved convenience for patients,” said study lead Dr Ana Luisa Neves, Advanced Research Fellow and Associate Director of our NIHR Imperial Patient Safety Translational Research Centre.
“We also learnt about the main challenges of using remote care, faced by both patients and doctors – digital exclusion from lacking access to technology, clinical uncertainty, potential delays in diagnosis and treatment, and unsuitability for certain types of consultations.
“The work also highlighted other challenges such as the lack of formal guidance, higher workloads, and technical difficulties. Unsurprisingly, digital exclusion and the potential to entrench existing health inequities were among the major concerns of the participants.
“We believe that listening to the GPs’ experience during the pandemic is especially valuable to understand how digital remote care can be safely delivered in the future. We hope we can learn together from this massive real-life experiment and use this opportunity to take the best technology has to offer and change primary care for the better.”
Much research has moved online during COVID-19, but that hasn’t stopped Lindsay and her co-researchers
World Mental Health Day is an opportunity to reflect on what needs to change, but also to celebrate the people who are working to make sure positive change happens. Like Dr Lindsay Dewa, IGHI Research Fellow and mental health expert.
We caught up with Lindsay to find out about her mental health research, her path into academia, and why she’s excited about what the future might hold. (more…)
“No test is better than a bad test,” said Matt Hancock.
While we may tire of hearing slogans, the principle here is important.
Coronavirus antibody tests have been hailed as a game-changer for the pandemic and a way forward as we traverse these uncertain times. Antibodies are Y-shaped immune molecules produced by the body in response to an infection. They latch onto the offender – such as coronavirus – in a bid to thwart it. Your body keeps a record of the encounter, so that if it comes across the same pathogen in the future, it can quickly make more antibodies and launch an effective attack.
This is the basis for hedging bets on antibody testing for coronavirus. The idea is that the tests will flag people who have already had the infection and therefore might have protection from getting it again. And so these individuals could potentially be afforded greater flexibility than those vulnerable to the disease.
But it’s not that simple.
Despite being known for under a year, this is arguably one of the most studied viruses ever. Yet it’s still new, and there are many unknowns. Crucially, we don’t yet know whether having antibodies can prevent future infection. Or, even if they do, how long this immunity lasts – a month, a year, many years? These are all questions we must answer before a potentially dangerous over-reliance is placed on these tests.
With so many caveats, why are researchers at Imperial leading a major study of community antibody testing? While the tests’ power to indicate immunity is – as yet – far from clear, they have important uses beyond this. Rather than focussing on individuals, looking at widespread patterns at the population level could help to monitor the evolution of the epidemic, which will have important implications for easing of restrictions such as social distancing.
Antibodies vs antigens
Currently the most accurate way to look for antibodies is to perform a lab test called an ELISA, on a sample of blood. Antibodies are very selective about what they stick to – specific molecules called ‘antigens’ (in this case, bits of the coronavirus). In an ELISA, a blood sample is mixed with coronavirus antigens that are ‘glued’ onto a test surface. If antibodies are present in the sample, they stick to the antigens and this binding leads to a detectable signal, most commonly in the form of a colour change.
These lab-based tests are accurate and can tell us the exact amount of antibody in a sample, but they’re complicated to perform, and require expensive, specialised labs. This means it’s not feasible to roll out this kind of antibody testing at a national scale, when labs are already overburdened. That’s why Imperial’s REACT study is looking at the possibility of using home testing kits instead.
“The big advantage is that the home testing kits are really cheap to produce, easy to distribute and store at room temperature, and they completely bypass the lab,” says Barney Flower, Clinical Research Fellow at Imperial and member of the REACT study team. “The beauty is that you get participants to do the leg work and carry out the tests themselves, so it’s less of a capacity issue when resources are stretched.”
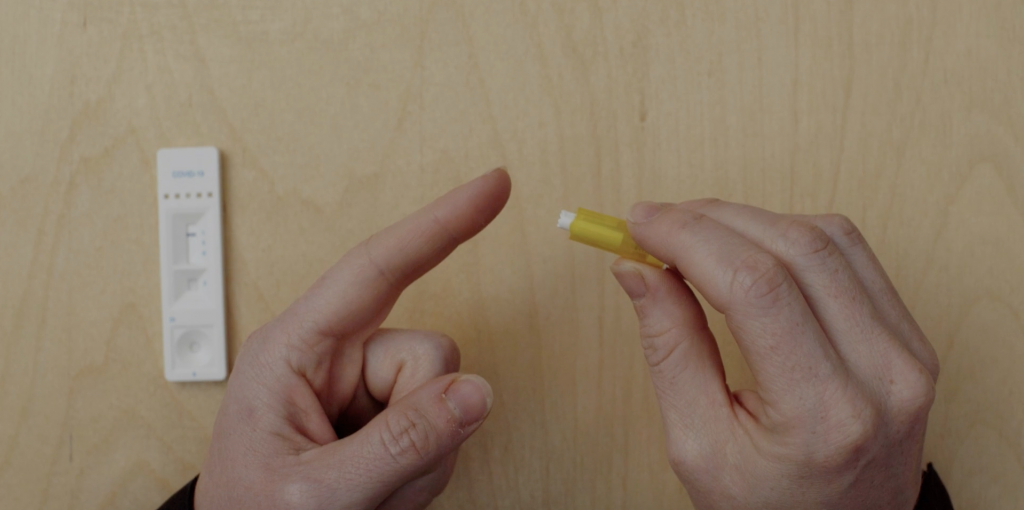
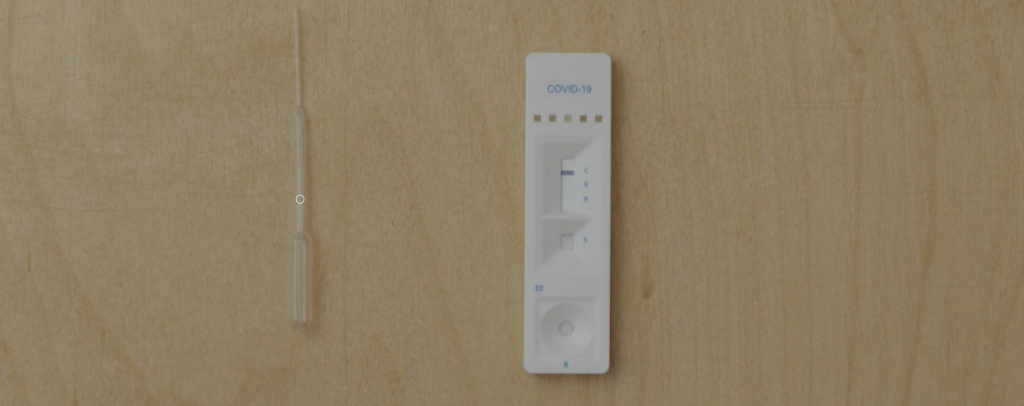
These home tests, called Lateral Flow Tests (LFTs), work in a similar way to ELISA, but everything is crammed into a small testing stick, which participants place a drop of blood onto. If antibodies are present, a signal will show up in a window on the testing stick, usually a coloured line.
The antibody testing kits display coloured lines depending on the result
A flooded market
By May of this year, already more than 200 of these LFTs had reached the market. However, there was no guarantee of their accuracy.
“The tests have been validated for use in laboratories, but in general their performance has been tested in small numbers of individuals, often fewer than 50 patients,” Barney says. “And these were usually individuals who were in hospital with COVID-19, so quite sick, and therefore more likely to have a strong immune response to the virus, producing lots of antibodies.”
This presents an issue, given that many people who have been infected with the coronavirus don’t have symptoms, and most don’t end up in hospital. So it’s critical to ensure that these tests work in this key group. And it’s also important to make sure that the tests perform well when they’re carried out by individuals themselves, not a trained technician – which is usually how they’re scrutinised in formal validation tests.
Antibody test results: true or false?
There are two main criteria that researchers use to assess how well an antibody test works. Its sensitivity is how well it picks up people who have been infected. If a test is 95% sensitive, for example, then out of 100 individuals who have had COVID-19, five will be wrongly identified as having not been previously infected (false negatives). Specificity, on the other hand, concerns the test’s ability to correctly identify those who were not infected. So if a test’s 99% specific, out of 100 people who haven’t had COVID-19, one will be wrongly identified as having been infected (a false positive).
In the UK, our regulator of medicines and medical devices (the MHRA), set out guidelines which stated that antibody tests need to be at least 98% sensitive to be able to guide decision-making in the clinic.
“The tests we’ve been looking at have been far below that,” Barney says. “So they’re no good at the individual level. But if we can find a test that’s really specific, we can make adjustments in our calculations and get a fairly accurate picture of the proportion of people who have antibodies at the population level.”
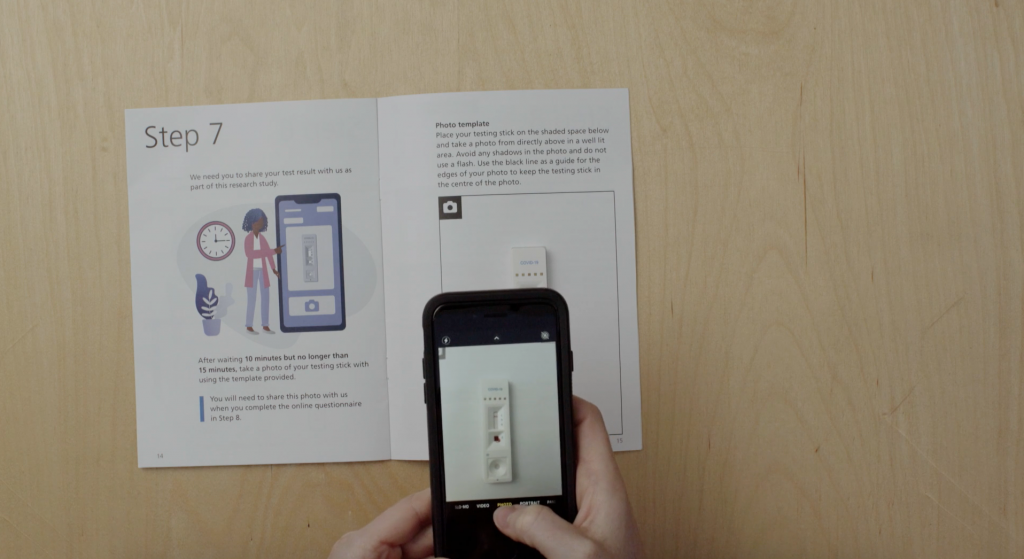
Study participants are asked to read the result of their test and submit a photograph so that researchers can review their interpretation
A testing conveyor belt
For the REACT programme, a team led by Professor Graham Cooke has been assessing a number of different commercially available tests, including the Wondfo test that the UK Government stockpiled early on in the epidemic. In the first phase, researchers carried out a small-scale study to test accuracy and usability (how well people can perform the test by themselves) on a group of around 270 healthy people, all NHS staff. Importantly, they’d all had a previous diagnosis of COVID-19 confirmed by a nose swab, but none of them had been hospitalised from the disease.
“The first test we tried out was throwing out negative results in four out of five participants – in a group who’d all had confirmed infection,” Barney says.
As well as testing the positive cases’ blood with the antibody kits, the researchers also performed an accurate lab ELISA to check if antibodies were detectable on the best test available. They found antibodies were present in more than 95% of cases.
They also tested the antibody kits on a batch of 500 blood samples taken from 2019 or earlier, i.e. preceding the pandemic and therefore COVID-19-free.
Together, this process is allowing the researchers to determine the tests’ sensitivity and specificity with a high degree of confidence.
“We’ve now developed a system where we can continually bring in new tests as they emerge, evaluate them on our bank of ‘known positive’ and ‘known negative’ samples, and if they look good we can test them in the clinic in more of a real-life scenario,” Barney says. “It’s like a lateral flow test conveyor belt.”
It’s how you use it
Another vital aspect of this work has been determining how usable these tests are by members of the public. Even if they perform well in controlled environments, they’re no good for use en masse if people can’t do them at home. A huge effort has been underway at Imperial, led by Prof Helen Ward, to involve and engage the public in this part of the project. Thousands of volunteers to date have given their time, offering valuable insight that’s not possible to gauge through lab testing alone.
While all of the LFTs work in the same way – placing a drop of blood onto a testing stick – there have been a number of issues with usability that this public involvement exercise has flagged up.
“This has been so important to highlight real issues with the tests,” Barney says. “One of the major things has been getting enough blood from the finger-prick, and successfully dropping this on the right part of the testing strip.”
At the start of the study, participants were provided with a plastic pipette to collect their blood after pricking their finger, which was then used to transfer a droplet of their blood onto the stick. But this soon proved a fiddly procedure, and now individuals are asked to place a drop of blood directly onto the test.
“We also found that health professionals tended to dive straight in and pay less attention to the instruction manual, and were therefore more likely to get it wrong!” Barney recounts. “Clear, simple instructions are so important!”
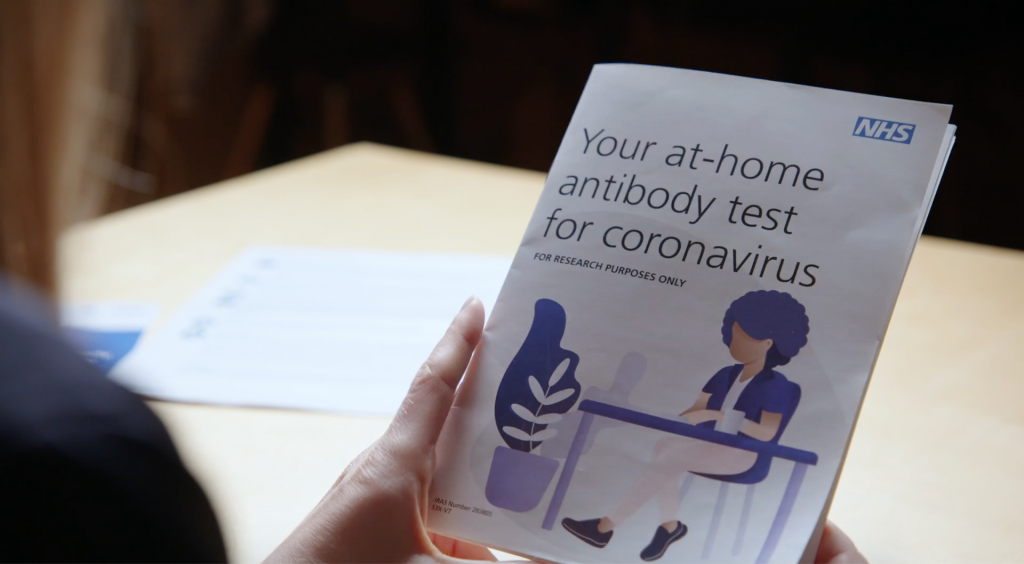
The leaflet to guide people through the at-home antibody test was developed with the public
Blood, spit, spots
While this research continues, the REACT team has narrowed down their hunt for the best home LFT. After analysing 11 different LFTs in the lab, they found the best tests could correctly identify individuals with coronavirus antibodies over 80% of the time, while also correctly ruling out those who don’t in more than 98% of tested individuals.
Based on these findings, the team selected and rolled out a finger-prick test to more than 100,000 people across England, who tested themselves at home in June and July. Covering all 315 local authorities to ensure a nationally-representative sample, this major study found that just under 6% of the population had antibodies to coronavirus and had therefore likely already had COVID-19. It also revealed that the virus hadn’t spread evenly across the country, disproportionally affecting key workers and Black, Asian and minority ethnic individuals.
Watch the video below for the study highlights:
Today we announced our findings of the world’s largest study on home coronavirus antibody testing. @imperialcollege researchers show that around 3.4 million people in England may have already had #COVID19, but that it hasn’t spread evenly across the country.
The team is continuing further testing of LFTs on a group of 5,000 key workers to gather more data. This particular piece of work is also investigating whether other methods could also be used for antibody testing, such as saliva samples or drops of blood dried on paper.
While this research can’t tell us anything about possible immunity levels, its offering is a greater understanding of how the epidemic is progressing, and who is at greatest risk from the infection.
“What this can help us understand is how many people have been exposed to the virus,” Barney says.
“Comparing these numbers to deaths and numbers admitted to hospital, in different populations and different parts of the country, will help plan for future outbreaks.
“However, it’s still important to say that we don’t know what these antibodies mean for individuals yet. Do they offer protection? And if so, for how long? The future of mass antibody testing rests on what we can learn from research like this.”