Almost half of all deaths in children under the age of five are linked to undernutrition. Most of these occur in the developing world. There is therefore an urgent need to address this pressing issue which costs the lives of millions of children every year. And as detailed below, the answer is not as simple as providing more food.
In a new Gut review, led by IGHI lecturer Dr Alex Thompson, scientists explore the role that technology could play in improving understanding, management and prevention of this complex condition, with a focus on low- and middle-income countries.
We caught up with Dr Thompson to find out more. (more…)
“We’re in this together.” One year ago, on 11th March 2020, the World Health Organization declared COVID-19 a global pandemic.
Back then, little over 100,000 cases had been reported globally. Today that number is 1,000 times greater and growing ceaselessly.
With a barely known virus rippling across the world, so too did fear and uncertainty spread as the WHO Director-General addressed all people and nations to make the declaration. Shifting the focus from COVID-19 to people and unity, Dr Tedros also sparked glimmers of optimism by emphasising that innovation and learning would be integral to saving lives and minimising the impact of the pandemic.
Innovation is the beating heart of IGHI, and we’re proud of our community that has joined this long and winding path of discovery in many different ways. A year on, our people reflect on their COVID-19 response journeys and impart the lessons they’ve learned along the way.
Read their stories below.
Tracking COVID-19 past and present – the REACT study
In April 2020 we launched the biggest and most comprehensive study of home coronavirus testing. With colleagues across the College, Imperial College Healthcare NHS Trust, and Ipsos MORI, the REACT programme has been testing hundreds of thousands of people across England every month to track infections past and present. Alongside understanding how many people are currently infected, REACT is identifying people who are most at risk of infection while offering a range of other important insights, such as antibody responses to vaccination. The programme has also worked closely with members of the public to ensure that the research is guided by people’s needs.
This work has been instrumental in the monitoring of England’s epidemic and offers robust, timely evidence on the evolving situation, which is continuing to shape the government’s response.
“One phrase has dominated Government pronouncements on the roadmap out of lockdown: ‘Data, not dates,’” said Professor Ara Darzi, REACT programme sponsor and co-director of IGHI. “And rightly so. The Covid crisis has caused terrible suffering, wrecking lives and livelihoods. But unless we understand it, we cannot defeat it.
“Among the most pressing questions over the last year have been how many people are currently infected with the virus, and how far has it spread through the population? REACT has been a key element of the effort to answer these questions, providing among the most accurate and up-to-date data on its progression across England.
“By regularly testing 160,000 randomly selected people every month, the study has played a vital role in informing the Government’s decision over when to impose lockdown and when to lift it.
“In doing so it has proved the central importance of accurate data gathering to control this and any future pandemic. We forget this lesson at our peril.”
Social distancing measures have helped keep the virus at bay, but not without cost. The loneliness and isolation that come with keeping people apart are negatively impacting people’s wellbeing, particularly so for those who depend on support from others in their everyday lives, such as people with dementia.
In response to this issue, our Helix Centre partnered with collaborators to develop a digital resource to help community groups create online networks as a way to maintain support and connection for people affected by dementia. Called Community Makers, the initiative is also building a toolkit of creative ideas for digital involvement, including how to reach people who may not have access to technology.
“Community Makers was a project that addressed a real-time need we saw in the people we were working with through our dementia research,” said Matt Harrison, senior designer at IGHI’s Helix Centre and project lead at Imperial. “People with dementia were some of the least able to adapt to lockdown measures and keep themselves isolated, yet very vulnerable to COVID.
“Collaborating daily with colleagues I have never met in person, at Alzheimer’s Society and University of Worcester, it has been inspiring to work with community groups across the country and see how they have adapted to using digital tools to support their members, and see how technology has evolved to match the need. However, the need is still not met, and there is much more to be done. The post-COVID world will be made up of the best of in-person and digital connections, and we are now seeking funding to help facilitate that change.”
Monitoring people’s changing attitudes and behaviours
Washing our hands regularly, taking public transport, avoiding meeting people outside of our household – many of the things we do affect our risk of COVID-19. Public health measures and campaigns have been designed to encourage people to behave in ways that reduce this risk, but how well are people sticking to them? And how are people’s attitudes in relation to the crisis changing over time?
Launched in March 2020 with YouGov, our ongoing COVID-19 health behaviour study is the largest of its kind, surveying thousands of people across the globe every month – half a million in total to date – to understand how citizens are responding to the pandemic. By making the findings freely available, and collaborating with a range of partners, our work is enabling decision-makers to tailor their response based on evidence.
“The stories that emerged, their common threads and their remarkable differences have helped many scientists, public health authorities, members of the press, government leaders and the public to come to grips with many of the driving forces behind the spread of COVID-19,” said Sarah P Jones, project co-creator and doctoral researcher at IGHI.
“When I look back across the year I’m struck by not the divisions sown between us, but by the overwhelming cooperation the world has generated.
“At the beginning of the pandemic I saw every new announcement as a rule, a constraint or a liberty taken away.
“But starting from the very first time YouGov returned our global survey results, I realised something incredible was happening in the world.
“Every hand washed, every mask worn, every metre of distance we placed between ourselves and others have been a gesture towards each other, a signal of respecting one another’s safety.
“I personally cannot wait to get back to hugging, to hearing stories in person and to caring for those I love who are still far away.
“But as we emerge from this cocoon the question on many peoples’ minds should not be “How can we get back to normal?” but rather “Is there anything we cannot accomplish together?”
Understanding the impact of the COVID-driven digital shift in primary care
Digital technologies have been poised to transform the delivery of health care for some time. When the pandemic hit, their promise was quickly put to the test as health systems were forced to shift much of their care from in-person to remote delivery.
Switching from face-to-face consultations to phone calls and video meetings has enabled services to continue while keeping both patients and healthcare staff safe. But what has been the impact for patients and professionals? Our international InSIGHT study has been working with global collaborators to explore this in primary care, using a survey to gather the perspectives of thousands of GPs across 20 countries.
“We were pleased to hear that GPs identified a range of benefits, including reducing COVID-19 transmission risks, guaranteeing access and continuity of care, greater efficiency, faster access to care, and improved convenience for patients,” said study lead Dr Ana Luisa Neves, Advanced Research Fellow and Associate Director of our NIHR Imperial Patient Safety Translational Research Centre.
“We also learnt about the main challenges of using remote care, faced by both patients and doctors – digital exclusion from lacking access to technology, clinical uncertainty, potential delays in diagnosis and treatment, and unsuitability for certain types of consultations.
“The work also highlighted other challenges such as the lack of formal guidance, higher workloads, and technical difficulties. Unsurprisingly, digital exclusion and the potential to entrench existing health inequities were among the major concerns of the participants.
“We believe that listening to the GPs’ experience during the pandemic is especially valuable to understand how digital remote care can be safely delivered in the future. We hope we can learn together from this massive real-life experiment and use this opportunity to take the best technology has to offer and change primary care for the better.”
Much research has moved online during COVID-19, but that hasn’t stopped Lindsay and her co-researchers
World Mental Health Day is an opportunity to reflect on what needs to change, but also to celebrate the people who are working to make sure positive change happens. Like Dr Lindsay Dewa, IGHI Research Fellow and mental health expert.
We caught up with Lindsay to find out about her mental health research, her path into academia, and why she’s excited about what the future might hold. (more…)
“No test is better than a bad test,” said Matt Hancock.
While we may tire of hearing slogans, the principle here is important.
Coronavirus antibody tests have been hailed as a game-changer for the pandemic and a way forward as we traverse these uncertain times. Antibodies are Y-shaped immune molecules produced by the body in response to an infection. They latch onto the offender – such as coronavirus – in a bid to thwart it. Your body keeps a record of the encounter, so that if it comes across the same pathogen in the future, it can quickly make more antibodies and launch an effective attack.
This is the basis for hedging bets on antibody testing for coronavirus. The idea is that the tests will flag people who have already had the infection and therefore might have protection from getting it again. And so these individuals could potentially be afforded greater flexibility than those vulnerable to the disease.
But it’s not that simple.
Despite being known for under a year, this is arguably one of the most studied viruses ever. Yet it’s still new, and there are many unknowns. Crucially, we don’t yet know whether having antibodies can prevent future infection. Or, even if they do, how long this immunity lasts – a month, a year, many years? These are all questions we must answer before a potentially dangerous over-reliance is placed on these tests.
With so many caveats, why are researchers at Imperial leading a major study of community antibody testing? While the tests’ power to indicate immunity is – as yet – far from clear, they have important uses beyond this. Rather than focussing on individuals, looking at widespread patterns at the population level could help to monitor the evolution of the epidemic, which will have important implications for easing of restrictions such as social distancing.
Antibodies vs antigens
Currently the most accurate way to look for antibodies is to perform a lab test called an ELISA, on a sample of blood. Antibodies are very selective about what they stick to – specific molecules called ‘antigens’ (in this case, bits of the coronavirus). In an ELISA, a blood sample is mixed with coronavirus antigens that are ‘glued’ onto a test surface. If antibodies are present in the sample, they stick to the antigens and this binding leads to a detectable signal, most commonly in the form of a colour change.
These lab-based tests are accurate and can tell us the exact amount of antibody in a sample, but they’re complicated to perform, and require expensive, specialised labs. This means it’s not feasible to roll out this kind of antibody testing at a national scale, when labs are already overburdened. That’s why Imperial’s REACT study is looking at the possibility of using home testing kits instead.
“The big advantage is that the home testing kits are really cheap to produce, easy to distribute and store at room temperature, and they completely bypass the lab,” says Barney Flower, Clinical Research Fellow at Imperial and member of the REACT study team. “The beauty is that you get participants to do the leg work and carry out the tests themselves, so it’s less of a capacity issue when resources are stretched.”
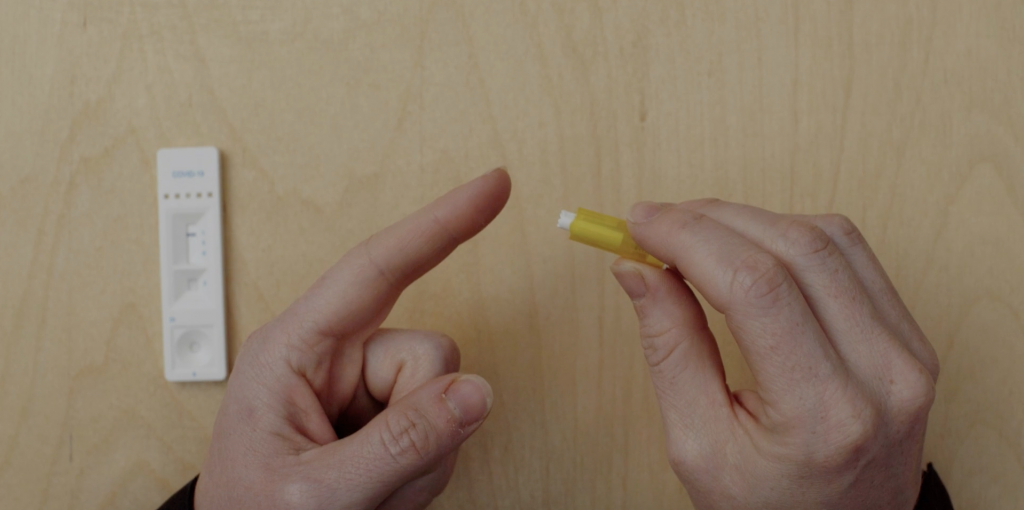
These home tests, called Lateral Flow Tests (LFTs), work in a similar way to ELISA, but everything is crammed into a small testing stick, which participants place a drop of blood onto. If antibodies are present, a signal will show up in a window on the testing stick, usually a coloured line.
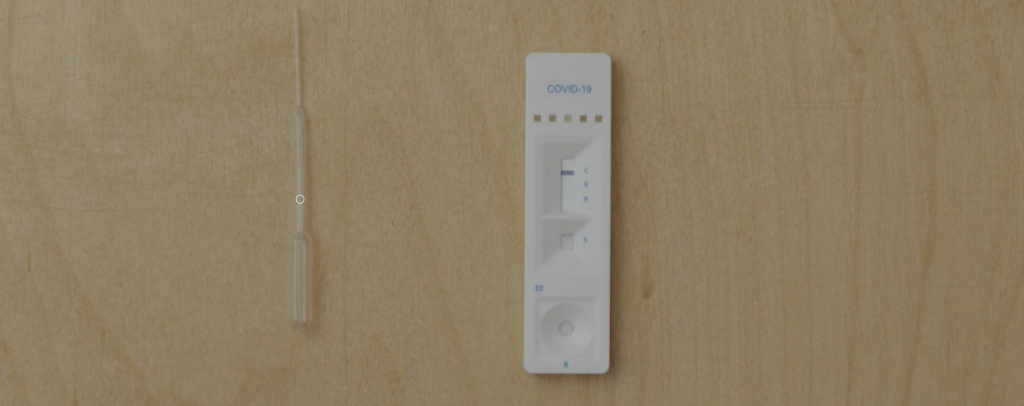
The antibody testing kits display coloured lines depending on the result
A flooded market
By May of this year, already more than 200 of these LFTs had reached the market. However, there was no guarantee of their accuracy.
“The tests have been validated for use in laboratories, but in general their performance has been tested in small numbers of individuals, often fewer than 50 patients,” Barney says. “And these were usually individuals who were in hospital with COVID-19, so quite sick, and therefore more likely to have a strong immune response to the virus, producing lots of antibodies.”
This presents an issue, given that many people who have been infected with the coronavirus don’t have symptoms, and most don’t end up in hospital. So it’s critical to ensure that these tests work in this key group. And it’s also important to make sure that the tests perform well when they’re carried out by individuals themselves, not a trained technician – which is usually how they’re scrutinised in formal validation tests.
Antibody test results: true or false?
There are two main criteria that researchers use to assess how well an antibody test works. Its sensitivity is how well it picks up people who have been infected. If a test is 95% sensitive, for example, then out of 100 individuals who have had COVID-19, five will be wrongly identified as having not been previously infected (false negatives). Specificity, on the other hand, concerns the test’s ability to correctly identify those who were not infected. So if a test’s 99% specific, out of 100 people who haven’t had COVID-19, one will be wrongly identified as having been infected (a false positive).
In the UK, our regulator of medicines and medical devices (the MHRA), set out guidelines which stated that antibody tests need to be at least 98% sensitive to be able to guide decision-making in the clinic.
“The tests we’ve been looking at have been far below that,” Barney says. “So they’re no good at the individual level. But if we can find a test that’s really specific, we can make adjustments in our calculations and get a fairly accurate picture of the proportion of people who have antibodies at the population level.”
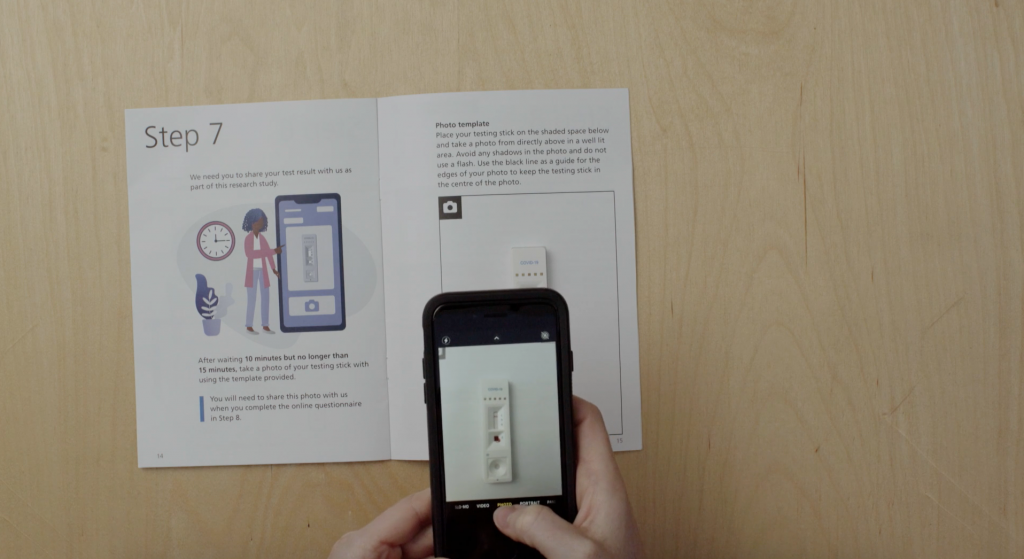
Study participants are asked to read the result of their test and submit a photograph so that researchers can review their interpretation
A testing conveyor belt
For the REACT programme, a team led by Professor Graham Cooke has been assessing a number of different commercially available tests, including the Wondfo test that the UK Government stockpiled early on in the epidemic. In the first phase, researchers carried out a small-scale study to test accuracy and usability (how well people can perform the test by themselves) on a group of around 270 healthy people, all NHS staff. Importantly, they’d all had a previous diagnosis of COVID-19 confirmed by a nose swab, but none of them had been hospitalised from the disease.
“The first test we tried out was throwing out negative results in four out of five participants – in a group who’d all had confirmed infection,” Barney says.
As well as testing the positive cases’ blood with the antibody kits, the researchers also performed an accurate lab ELISA to check if antibodies were detectable on the best test available. They found antibodies were present in more than 95% of cases.
They also tested the antibody kits on a batch of 500 blood samples taken from 2019 or earlier, i.e. preceding the pandemic and therefore COVID-19-free.
Together, this process is allowing the researchers to determine the tests’ sensitivity and specificity with a high degree of confidence.
“We’ve now developed a system where we can continually bring in new tests as they emerge, evaluate them on our bank of ‘known positive’ and ‘known negative’ samples, and if they look good we can test them in the clinic in more of a real-life scenario,” Barney says. “It’s like a lateral flow test conveyor belt.”
It’s how you use it
Another vital aspect of this work has been determining how usable these tests are by members of the public. Even if they perform well in controlled environments, they’re no good for use en masse if people can’t do them at home. A huge effort has been underway at Imperial, led by Prof Helen Ward, to involve and engage the public in this part of the project. Thousands of volunteers to date have given their time, offering valuable insight that’s not possible to gauge through lab testing alone.
While all of the LFTs work in the same way – placing a drop of blood onto a testing stick – there have been a number of issues with usability that this public involvement exercise has flagged up.
“This has been so important to highlight real issues with the tests,” Barney says. “One of the major things has been getting enough blood from the finger-prick, and successfully dropping this on the right part of the testing strip.”
At the start of the study, participants were provided with a plastic pipette to collect their blood after pricking their finger, which was then used to transfer a droplet of their blood onto the stick. But this soon proved a fiddly procedure, and now individuals are asked to place a drop of blood directly onto the test.
“We also found that health professionals tended to dive straight in and pay less attention to the instruction manual, and were therefore more likely to get it wrong!” Barney recounts. “Clear, simple instructions are so important!”
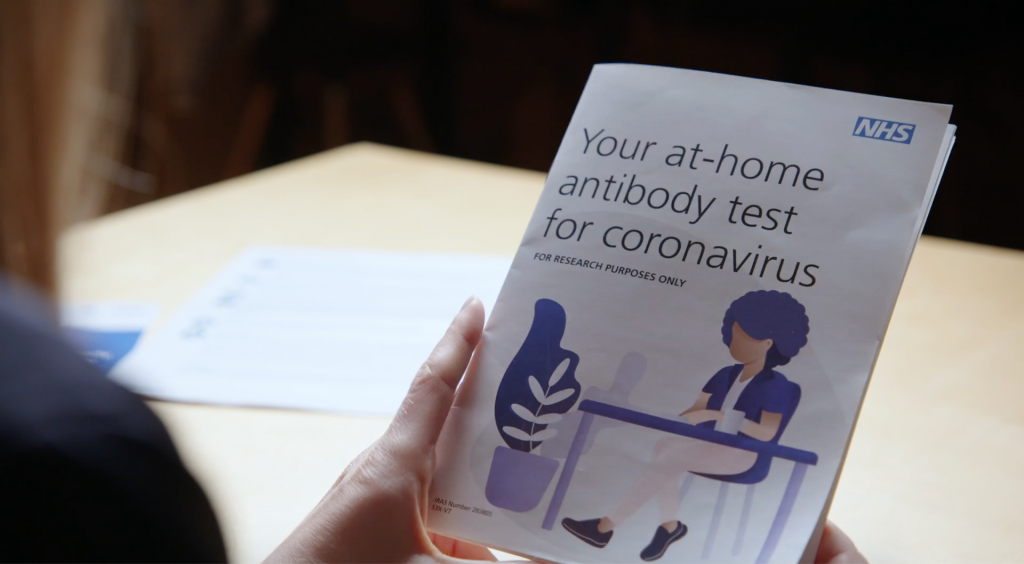
The leaflet to guide people through the at-home antibody test was developed with the public
Blood, spit, spots
While this research continues, the REACT team has narrowed down their hunt for the best home LFT. After analysing 11 different LFTs in the lab, they found the best tests could correctly identify individuals with coronavirus antibodies over 80% of the time, while also correctly ruling out those who don’t in more than 98% of tested individuals.
Based on these findings, the team selected and rolled out a finger-prick test to more than 100,000 people across England, who tested themselves at home in June and July. Covering all 315 local authorities to ensure a nationally-representative sample, this major study found that just under 6% of the population had antibodies to coronavirus and had therefore likely already had COVID-19. It also revealed that the virus hadn’t spread evenly across the country, disproportionally affecting key workers and Black, Asian and minority ethnic individuals.
Watch the video below for the study highlights:
Today we announced our findings of the world’s largest study on home coronavirus antibody testing. @imperialcollege researchers show that around 3.4 million people in England may have already had #COVID19, but that it hasn’t spread evenly across the country.
The team is continuing further testing of LFTs on a group of 5,000 key workers to gather more data. This particular piece of work is also investigating whether other methods could also be used for antibody testing, such as saliva samples or drops of blood dried on paper.
While this research can’t tell us anything about possible immunity levels, its offering is a greater understanding of how the epidemic is progressing, and who is at greatest risk from the infection.
“What this can help us understand is how many people have been exposed to the virus,” Barney says.
“Comparing these numbers to deaths and numbers admitted to hospital, in different populations and different parts of the country, will help plan for future outbreaks.
“However, it’s still important to say that we don’t know what these antibodies mean for individuals yet. Do they offer protection? And if so, for how long? The future of mass antibody testing rests on what we can learn from research like this.”
Digital technology has been poised to transform the way that healthcare is delivered. Yet uptake and implementation has been slow; in the UK alone for example, almost a quarter of hospitals still use paper rather than electronic records.
But when COVID-19 hit, health systems were forced to rapidly adapt and use technology to deliver care remotely, where face to face appointments were no longer possible. While it’s impossible to predict when the COVID crisis will be over, will remote care become the ‘new normal’ post-pandemic? And if digital-first health technologies are here to stay, what are the implications for patients?
Newly launched IGHI research, supported by Imperial’s COVID-19 Response Fund, will explore these important questions. We caught up with project lead, IGHI Research Fellow Dr Ana Luisa Neves, to find out more about the work and what it hopes to achieve.
What are digital-first health technologies?
“These are all means in which the patient’s first point of contact is through a digital channel, rather than face-to-face. For example, phone and video consultations, online services, and mobile apps.”
Why are you interested in these?
“Our idea is that digital technology can help tackle challenges that we had before COVID hit. Like making care more accessible and affordable, and reaching groups of people who may not be confident going to a doctor or nurse.
“Right now we’re in the middle of a massive real-life experiment, which has pushed this closer to reality. We will resume normality at some stage, however it may look. But what can we take from this experience so that we can continue using these models in a better way?”
What are you hoping to find out about these technologies?
“We want to understand the patient experience. In principle these technologies should improve accessibility, but that may not turn out to be true – or at least not true for everyone. So we’ll explore the potential barriers to healthcare access, whether some individuals or groups are somehow excluded from these technologies.
“We also want to look at patients’ attitudes and perceptions. In what circumstances do they want to use digital technologies? How do patients want these to move forward? When do they think that digital tech may work better than more traditional models of care, and how can we create conditions for that to happen?”
And how are you going to answer those questions?
“This work sits within a broader program of work that’s also looking at GPs’ views of these technologies. That’s using a global survey and focus groups, involving 18 countries. We’ll be replicating this method but looking at patients’ perspectives instead.
“We want to make sure we get nationally-representative samples from countries and information about demographics, as well as ‘digital literacy’. Part of digital literacy covers technical aspects, such as Internet access, but also individuals’ ability and experience using digital tools.”
Do you have any assumptions about what you might find?
“I expect we’ll find that certain groups feel excluded. Evidence has shown that elderly individuals, for example, or those with lower digital literacy are less likely to use these technologies. We want to understand what we can do to make it easier for them.”
How will you apply your findings to healthcare settings?
“We’re hoping to bring together the findings from both GPs and patients, and then consider how we can make these technologies better for the future. We’ll then develop a framework for recommendations, a ‘toolkit’ that healthcare professionals can use to support decision-making. For example, when triaging patients, the framework could help doctors identify when digital technologies may be useful and appropriate. This could help doctors decide whether to offer digital solutions as part of patient care, post-COVID-19.”
Grappling with a novel virus that reared its ugly head barely six months ago, the world is facing many uncertainties. The SARS-CoV-2 virus is proving unpredictable and the pandemic is fast-moving. But one thing we do know is that older people bear the brunt of the impacts of COVID-19. The elderly are disproportionately affected, with those over 65 accounting for some 80% of hospitalisations due to the disease. And one in five over-80s with COVID-19 will need to go to hospital, compared with one in 100 individuals under 30. (more…)
In the midst of a global pandemic, our people are continuing their endeavour to improve health and care. In this new series, we’re speaking to our IGHI community to find out how they’re adapting to working life amid coronavirus, and the unique opportunities and challenges this has presented them. (more…)
Caroline, second from the left, talks about her experience of being involved in our research at a symposium on patient safety.
Research is our bread and butter at IGHI. It lets us explore problems, ask questions, test ideas, make mistakes and learn from them. And after all that, find the right solutions to the issues we’re trying to address in healthcare.
None of this would be possible without people. But not only the brilliant researchers who are the driving force behind our progress. The patients, carers, public and healthcare professionals who devote their time to get involved and be part of our research play an invaluable role in what we do, too. It is through their knowledge and lived experience that we know we’re asking the right questions and chasing the right solutions.
This International Clinical Trials Day, we want to highlight why being involved in research is vital to make progress in healthcare, and shine a light on some of the people who are doing just that.
Caroline, right, presenting findings of the research she carried out with Lindsay, left
Caroline’s story
“I was studying social sciences in London when I first got involved in research at IGHI. I’d been wanting to gain some experience in carrying out research, beyond filling out forms and surveys. I’m really interested in mental health and try to keep my finger on the pulse with what’s out there. So when this opportunity landed in my inbox, looking for young people with lived experience of mental health difficulties to take part in a project as co-researchers, it immediately struck my interest.
“The study was exploring the use of technology to detect deteriorating mental health in young people. We were involved in every stage of the project, helping to shape the work in a way that was meaningful. Sometimes it can feel like involvement is a bit of a tokenistic gesture to fulfil the criteria of a grant, but Lindsay and Anna, the research lead and involvement manager, never gave me that impression. By involving us, they wanted to make sure that the research was asking the right questions, and that it was relevant and of interest to the young people she’s seeking to help through her work.
“After helping to guide the direction of the research, we were trained to carry out interviews with young people with mental health difficulties, and then to code the transcripts and help analyse them. We even attended conferences and shared our findings at various events, so we really got to take part from start to finish. That meant I could really see the impact of the work and how everything fits together.
“It also really impacted me; knowing you’ve played a part in something that will likely affect others going through what you’ve been through is a really rewarding experience. And off the back of this project, I’ve actually started computer coding and will be starting a master’s in computer science.
“Before I joined this research project, I wasn’t really sure of the difference I could make. But I was so wrong! I worried my contributions would be the obvious thing to say, but I realised having that lived experience really does add another perspective that’s needed in research. I would definitely do it again and encourage others to do so – you really can make a difference.”
Anna’s story
Anna engaging with the public at one of our pop-up events. Credit: James Retief
“I’m the Patient and Public Involvement and Engagement (PPIE) Lead at IGHI. My role is to support the meaningful involvement of patients, carers and the public in research.
“It’s great to see how people like Caroline have not only impacted the research, but also gained from the experience, including learning new skills and growing in confidence. That’s why it’s so important that engagement and involvement in research continues despite the current crisis. Although COVID-19 has meant that we’ve had to change the way that we do this, we’re learning a lot and finding that involving people virtually can still be a really valuable and successful process.
“For online meetings, for example, we use ice breakers like “What’s your favourite lockdown TV show or book?” to help remove hierarchy and find some common ground, before we get the group to work on a task together. We’re using live captioning on our online platforms so people can read what is being said as well as listen, which has not only been useful for those with hearing loss, but also helps visual learners to reflect more on what is being said.
“Due to not being in person to read body language or take people outside for a chat, there is a greater need to ensure appropriate safeguarding. For example, we offer to chat to people individually before the meeting and introduce them to the online platform, so they will be familiar with at least one person. For sensitive topics or with vulnerable people, we have clinicians either in the meeting or on-call (to support people, as needed). We also ask individuals to provide a friend/family member’s contact details and signpost to appropriate support services (e.g. SHOUT crisis textline).
“We’re also thinking about ways to involve seldom heard groups during COVID-19, for example by providing dongles, as people might not have access to WiFi or unlimited data. We recognise not everyone wants to, or is able to, interact online. We want to build on existing community groups (e.g. through a buddy scheme or phoning rotas), but we also understand people might have more immediate needs to tend to.
“My colleagues and I are very grateful to the amazing, altruistic people who, although some of their situations might not improve, want to be involved in research to help others. We’re glad to hear people enjoy the experience of giving something back to the NHS. I enjoy seeing researchers, clinicians and public members learning from each other and, particularly now, learning together during this pandemic.”
In the midst of a global pandemic, our people are continuing their endeavour to improve health and care. In this new series, we’re speaking to our IGHI community to find out how they’re adapting to working life amid coronavirus, and the unique opportunities and challenges this has presented them. (more…)
Empty supermarket shelves have become synonymous with life amid coronavirus.
But the impact of the pandemic on food security goes far beyond the common frustrations of stockpiling driven by fear and a scarcity of pasta.
Restaurants and catering outlets have closed, food markets have drawn their shutters, social distancing and sickness have massively burdened workforces, and restrictions on movement have created a chink in the supply chain. All of this has created immense pressure on supermarkets that are having to cope with the ever-increasing demands, on farmers who are losing their clientele and are unable to distribute their produce, and on families who struggle to put food on their plates.
With food, nutrition and health inextricably linked, we spoke with Dr David Nabarro, IGHI Co-Director and food systems expert, to explore this complex and pressing situation further and find out what it could mean for individuals, communities and governments across the world.
Is food security amid coronavirus being given due attention?
Dr Nabarro, WHO Special Envoy on COVID-19. Photo by Owen Billcliffe
“Every community needs to focus on food and other essential requirements that are becoming harder to access as a result of both the pandemic itself, and the containment measures that countries are having to adopt.
“These containment measures are not optional and are the only way to get on top of this pandemic. But they will interrupt the economy. And they are also driving a rapid increase in hunger in all regions across the world, particularly in developing countries, as poor people on daily wages or working in the informal sector are unable to collect the cash they need to buy their essentials for life.
“This is being exacerbated by anxiety-driven stockpiling that is causing prices of food to rise; in some areas we’ve witnessed a 5 or 6-fold increase in the rise of essential products like cooking oil and flour.
“This is a global issue, but it’s worse in poor settings, and it’s occurring with great speed. This is putting even more urgency on the need to establish public health defences everywhere, so that life can restart.”
What about other vulnerable groups?
“Many school children get essential food intake from their school meals. With schools closed, these children are not receiving this valuable nutrition. This also means that households dependent on this free food are having to find the resources they need to feed their children.
“The same applies to old people receiving food support, such as ‘meals on wheels’, which may have stopped. So households are again having to find the extra cash to feed older people, too.”
Photo by Tra Tran on Unsplash
With governments fighting to prevent their economies from collapsing, is the onus being passed on to charities?
“In the past, many poorer people received a lot of support from NGOs, but these organisations are reporting a massive drop in their income. This is coming at a time when the world is going to depend on them more and more, and their capacity to respond will be limited. This is adding to an already massive problem.
“We are seeing huge increases in food insecurity and hunger, and they are only anticipated to worsen. If people can’t get food they will get frustrated, and they will move to places where they can find food. If they are prevented from doing so because of lockdowns, then this could cause unrest.
“There is therefore an urgency to sort this out, and I am engaging with people who are very focussed on this.”
And what about the farmers producing this food, how will they cope?
“Farmers will likely have difficulties accessing the things they need to produce food – seeds, fertilisers, etc. Farmers also need labour on their land, but worldwide restrictions on movement are creating problems sourcing workers. Looking ahead, this will generate supply issues.
“Farmers are also coping with a sudden crash in their markets due to restaurant closures, and with distribution issues due to restrictions on movement across and between countries, meaning perishable goods like fruits and vegetables are left to rot.
“All of these factors individually can make massive shocks to food systems. But taken together, this problem is huge, and it’s global. It is urgent we do something about it. And the only way we can get out of this is by concerted action and ensuring good quality public health in all communities.”
Photo by Kelly Sikkema on Unsplash
Who needs to take action to improve food security?
“Everybody has a role. Local authorities need to identify where there is hunger and provide targeted cash support. To prevent profiteering, local governments must also ensure that increases in the price of food are justified.
“Governments also need to make sure that people who work in the food sector are considered essential, like those who work in health. Finally, we must help farmers. Those falling short of cash as they are unable to distribute their food should receive help. We’re already talking to businesses about changing their distribution methods, shifting away from central distribution points to mobile methods that can more easily shift key items.
“But the most important thing is to know where people are hungry or likely to be, and making sure that they get support.”
What about us – what can we as citizens do to help?
“We all need to be prepared and willing to help where we can. Even in the most affluent societies, this kind of crisis can tip people over the edge into poverty. We need to be aware of this. And we need to keep giving to NGOs, who are experiencing a huge income drop. If we trust them, we should contribute, as they are able to get essential resources to people all over the world.
“And when this situation ends, we should revisit how we relate to farmers. They are so vital. Much like health workers, they have not always been treated with the respect that they deserve.”
Dr Nabarro is a WHO Special Envoy on COVID-19. He curates the Food Systems Dialogues and in 2018 won the World Food Prize In recognition of his successful leadership activities to galvanize policy-makers to prioritise food and nutrition.