In the midst of a global pandemic, our people are continuing their endeavour to improve health and care. In this new series, we’re speaking to our IGHI community to find out how they’re adapting to working life amid coronavirus, and the unique opportunities and challenges this has presented them.
Right now, we’ve never been more grateful for the health and care workers who are tirelessly demonstrating their dedication to our health and wellbeing.
Supporting our health system, too, are many unsung heroes working away from the frontline. People who may have hung up their stethoscopes, but with the same determination to improve health and care.
Like Drs Jack Halligan and Natalia Kurek at IGHI, who both left medicine but are staying at the forefront of healthcare in different ways.
We caught up with Jack and Natalia to find out about their careers post-medicine, how they’re applying what they learnt in medical school, and what the COVID-19 crisis means for their roles. (more…)
In a matter of mere months, a new virus has completely changed the world. In the trail of destruction that coronavirus is causing, it has rudely propelled many of us into a new way of working.
Offices have closed, laboratories shut their doors, classrooms and lecture theatres emptied. But the world has not ground to a halt – the show must go on. At IGHI, our researchers are continuing their endeavour to improve health and care. In this new series, find out how our people are adapting to working life amid coronavirus, and the unique opportunities and challenges this has presented them. (more…)
It was Christmas time three years ago when Amy experienced a stroke. Amy was enjoying her retirement, having spent her career working in publishing. But the stroke took away her independence, paralysing her left arm such that she needed full-time care. This isn’t an uncommon outcome: some 80% of people experience difficulty using their arms after a stroke.
Amy spent the next four months in hospital, the beginning of a long road to recovery.
“The rehabilitation I received in hospital mainly focused on walking, but it was my hand that I really needed help with,” she says.
“And I wasn’t told that if I didn’t use my hand that I would lose function of it.”
When Amy returned home she needed full-time care and regular rehabilitation sessions. But with an overstretched health system burdened by an ageing population, Amy wasn’t able to access the recovery support she required at home.
“I was glad to get out of hospital, but I couldn’t get the help I needed and felt very hard done by,” she says. “I had to take charge of my own recovery.”
Spotting gaps in stroke services
Amy joined a local network called LEGS (Local Exercise Groups for Stroke), a charity that offers physiotherapy-led rehabilitation for stroke survivors. It was here that she met Ella Gibbs and Gianpaolo Fusari from our Helix Centre, who were working on a solution to help people like Amy.
“Stroke is the leading cause of disability in the UK, so we were really motivated to work in this area and find out where we could use design to make a difference to people’s lives,” says Gianpaolo, senior designer at Helix, an innovation lab for healthcare.
“We wanted to learn more about what happens both in the hospital and in the community, so we shadowed teams of therapists on wards, linked up with various charities and also observed rehabilitation sessions in the home environment.”
It was the latter scenario where Gianpaolo realised there was a major gap to be filled.
“We followed early-support discharge teams, the therapists who go to people’s homes five days a week for 45 minutes to do intensive therapy,” he says.
“It’s a really great service, but only about 20-30% of eligible people receive it because there aren’t enough therapists to go around.”
A numbers game
The team ran workshops with patients and healthcare professionals to further flesh out people’s needs after stroke and better understand their feelings. It became clear that the lack of help at home was a real roadblock in people’s recovery.
“People felt unsupported after their formal rehabilitation programmes ended,” says Ella, physiotherapist and clinical researcher. “They were afraid to do some exercises at home for fear of injuring themselves. And they didn’t have any way of monitoring their own progress. The same goes for the therapists, who couldn’t see whether their patients were sticking to their exercises between sessions.”
Evidence suggests that stroke survivors need to perform hundreds of exercise repetitions every day to recover the function of their affected limbs. But even for those fortunate to be eligible for support at home, typical therapy sessions simply aren’t long enough to achieve those kinds of numbers. So rather than looking for an unlikely solution in these narrow windows, the Helix team began to focus on life outside of therapy. They wanted to help people help themselves – empowering them to take charge of their own recovery.
“There’s increasing emphasis on this self-management aspect of treatment for people with longer-term conditions,” says Jennifer Crow, an occupational therapist at Charing Cross Hospital who has been working with Helix on the project.
“Because people aren’t going to get a therapist’s help every time they need to do something. There simply aren’t enough of us. I believe self-management has to be the way of the future.”
A recipe for rehabilitation
Working with some 200 patients and healthcare professionals like Amy and Jennifer, the Helix team created a digital tool – OnTrack Rehab – that enables self-management of stroke recovery.
This platform couples a smartwatch app with tailored coaching to help people own their rehabilitation journey at home. The app works like a step counter. It tracks minutes of arm activity through an algorithm developed specifically for stroke survivors, whose arm movement differs from healthy individuals’.
“That’s the ‘secret sauce’ of our innovation,” says Gianpaolo.
The device displays these minutes to the user, alongside a daily goal and what they achieved the previous day. The app also sends the user tailored messages – depending on how active they are – to motivate and encourage them.
“It’s great – it reminds you to use your hand,” Amy says. “I think you need constant reminding that it’s there and needs to be used. I think it’s helped me to be more aware of that.”
Earlier versions of OnTrack showed users much more information. But testing sessions showed that people found it overwhelming and difficult to make sense of.
“What really struck me was how the Helix team really listened. Not just to us, the therapists, but to the patients as well,” Jennifer says. “Throughout this project they’ve always taken on board our suggestions, so that the next time we see them, they’ve made appropriate iterations. So much other research is done without any prior consideration of patients’ actual needs, which is so important.”
No single silver bullet
OnTrack shares the activity data it gathers not only with the users themselves, but also with their therapists. This offers a window into what happens between therapy sessions. The OnTrack team also uses this information to provide regular, tailored coaching sessions, which the therapists consult on.
By motivating people to better engage with their rehabilitation at home, OnTrack hopes to complement therapists. And ultimately, reduce the need for therapy sessions, which are in scarce supply.
Results from a pilot study in 2018 with 10 people showed an average increase in activity of 20%, which equates to roughly an extra hour of arm activity per day. While promising, the team can’t be sure that this improvement was due specifically to OnTrack. That’s why they’re now carrying out a more robust feasibility study with a larger number of patients and an independent evaluation.
The road ahead
Despite the years of research and development so far, it’s still early days for OnTrack. The team has more to do to refine the product and its features. They also need to demonstrate its impact on rehabilitation outcomes at scale. But if trials support its use, Gianpaolo has high hopes for the platform.
“In the short term, we want to see how it can integrate with NHS practice, becoming part of the services offered to stroke survivors here and hopefully in other countries in the future,” he says. “We also want to explore whether we can adapt OnTrack for rehabilitation in other areas. For example people living with Parkinson’s disease.”
The OnTrack team is excited for the road ahead and to helping many more people like Amy recover from stroke.
Cancer survival is improving and today, half of people diagnosed will survive their disease. This is thanks to research. Research that’s guiding governments to change their policies, underpinning awareness campaigns and educational initiatives, turning discoveries into treatments and prevention measures.
But there’s still much to be done to help more people survive, by catching the disease earlier and developing better treatments.
This World Cancer Day, and as part of our celebrations to mark IGHI’s 10th anniversary this year, find out how our researchers are working to make that happen. Join us in exploring some of our projects that could lead to better detection, diagnosis and treatment of cancer.
Using AI to help spot breast cancer
We’re helping to prove the potential for artificial intelligence to improve breast screening.
Mammograms use x-rays to image breast tissue. Photo by National Cancer Institute on Unsplash
IGHI is part of a collaboration – including DeepMind and Google Health – which is training computers to identify tumours in mammograms using a technique called machine learning. The team’s recent study, published in Nature, found that their AI system was as good as doctors at picking up cancers – and in some cases even outperformed them.
Breast screening involves taking x-ray images, or mammograms, of breast tissue which are then analysed by human experts. While screening continues to help save lives by picking up cancers earlier, sometimes tumours are missed. It can also lead to unnecessary treatment for tumours that wouldn’t have gone on to do any harm. That’s why our researchers are examining whether artificial intelligence could reduce the rate of error in the analysis of breast screening, and ultimately improve the management of breast cancer.
“We hope this work could minimise the burden of breast cancer in the UK and internationally,” says Mr Hutan Ashrafian, study author and IGHI scientific advisor. “Not only that, but we also believe this system has the ability to support clinicians by freeing up resources and allowing them to spend more time with patients.”
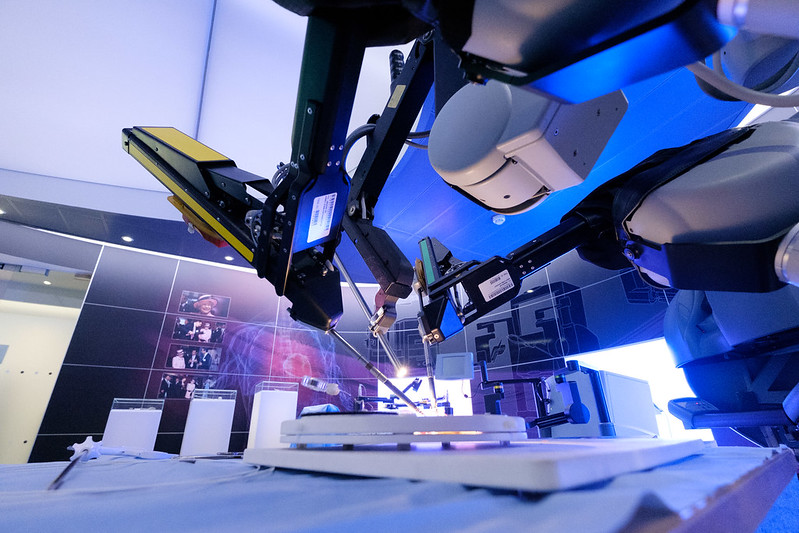
Robots for safer brain tumour surgery
Our researchers are working to make brain tumour treatment more precise, with the assistance of a bespoke intelligent robotic platform.
Researchers led by Dr Stamatia Giannarou from our Hamlyn Centre are integrating a number of imaging techniques and robotic instruments to develop a system that can more accurately characterise brain tumour tissue, and distinguish this from surrounding healthy tissue. In doing so, not only could the platform enable more accurate diagnosis, but it could also guide treatment decisions and help surgeons remove more of the cancerous tissue.
Brain tumours are very difficult to treat and survival remains stubbornly low. Surgery is the mainstay of treatment for many brain tumours, but being surrounded by delicate tissue makes the procedure particularly problematic. Surgeons can’t afford to remove too much tissue or risk serious side effects, yet remove too little and the treatment will be ineffective. Giannarou’s system hopes to change this.
“I’m passionate about contributing to a highly challenging research area, where we need significant advances in robotic vision to be able to navigate challenging and dynamic environments like the brain,” she says.
Supporting decision-making for suspect cancer
We’re launching a new project to guide the development of tools that are designed to support GPs’ decisions when managing patients with suspect cancer.
Cancer risk tools are algorithms that combine certain risk factors – like age and smoking status – with tell-tale symptoms to work out the probability of a person being diagnosed with cancer within a specific timeframe. Many patients present with symptoms that could indicate cancer, so these tools assist GPs in their decisions on who to investigate and refer.
Dr Olga Kostopoulou, research lead from our NIHR Patient Safety Translational Research Centre, will be investigating how these algorithms interact with GPs’ clinical judgment. She’ll be assessing things such as user trust and control, and looking at other concerns from GPs which could influence their decisions for urgent referral.
“The project aims to provide empirical evidence on these issues,” says Dr Kostopoulou. “And, in doing so, contribute to the currently expanding knowledge base about how such tools should be designed and introduced in clinical practice.”
Imaging to detect and track advanced disease
IGHI researchers are developing an imaging tool that they hope could detect or diagnose changes in cancer that has spread, or metastasised.
Endoscopies are a commonly used investigative technique, which traditionally relies on white light to image tissue inside the body. Prof Dan Elson from our Hamlyn Centre is testing out a different type of endoscopic imaging, called Polarization- and Multispectral-resolved Endoscopy. This uses different properties and wavelengths of light to reveal more information about tissues than is possible with traditional techniques, which can essentially only capture what the naked eye can see.
Prof Elson is investigating whether this type of imaging could help detect and characterise metastases in the tissue that lines the abdomen (peritoneum). For this work, they’re collaborating with the PIPAC trial that’s testing out a new treatment for advanced bowel cancer.
“The PIPAC trial is a good setting for us because the team regularly performs biopsies which we can image in the operating theatre,” says Prof Elson. “We also have the opportunity to image in vivo at different phases of treatment, potentially in the same patient.” Ultimately, doing so could help guide decisions in the clinic.
Making tissues glow to improve breast cancer surgery
Scientists at our Hamlyn Centre are developing an imaging system based on fluorescence that could help guide breast-conserving surgery.
They’re using a fluorescent dye that could help highlight differences between healthy and cancerous tissue, and a special camera system that can image these characteristics. The researchers hope this work could make the treatment more accurate by enabling surgeons to see tumours during surgery, reducing the likelihood of cancerous tissue being left behind.
“By making it easy for the surgeon to see both the location of the tumour and the extent to which it invades, our goal is to eliminate the risk that women require further surgery as the first operation did not remove all of the tumour,” says Clinical Research Fellow Dr Martha Kedrzycki, who is recruiting patients onto a trial that’s testing the system. “This technology could also be extrapolated for use in other cancers, aiding surgeons by highlighting targeted tissues.”
People complain for a variety of reasons. But international evidence consistently finds that most people complain to prevent incidents from happening to others – they want to see change as a result, when they feel something isn’t right. Making a complaint can therefore be an empowering process, if people know – or feel – that their actions could make a difference.
Dealing with complaints is an important learning process for those that the complaint is directed against, but also the institution more widely. They can highlight problems that may have otherwise slipped through the net, prompting action that can prevent the same mistakes happening again and affecting more people.
That’s why complaints are such a valuable resource for health systems. They’re a gold mine of information that represents people’s unfettered thoughts, feelings and real experiences with health care, representing an important opportunity to reflect, learn and improve.
But they can also be messy.
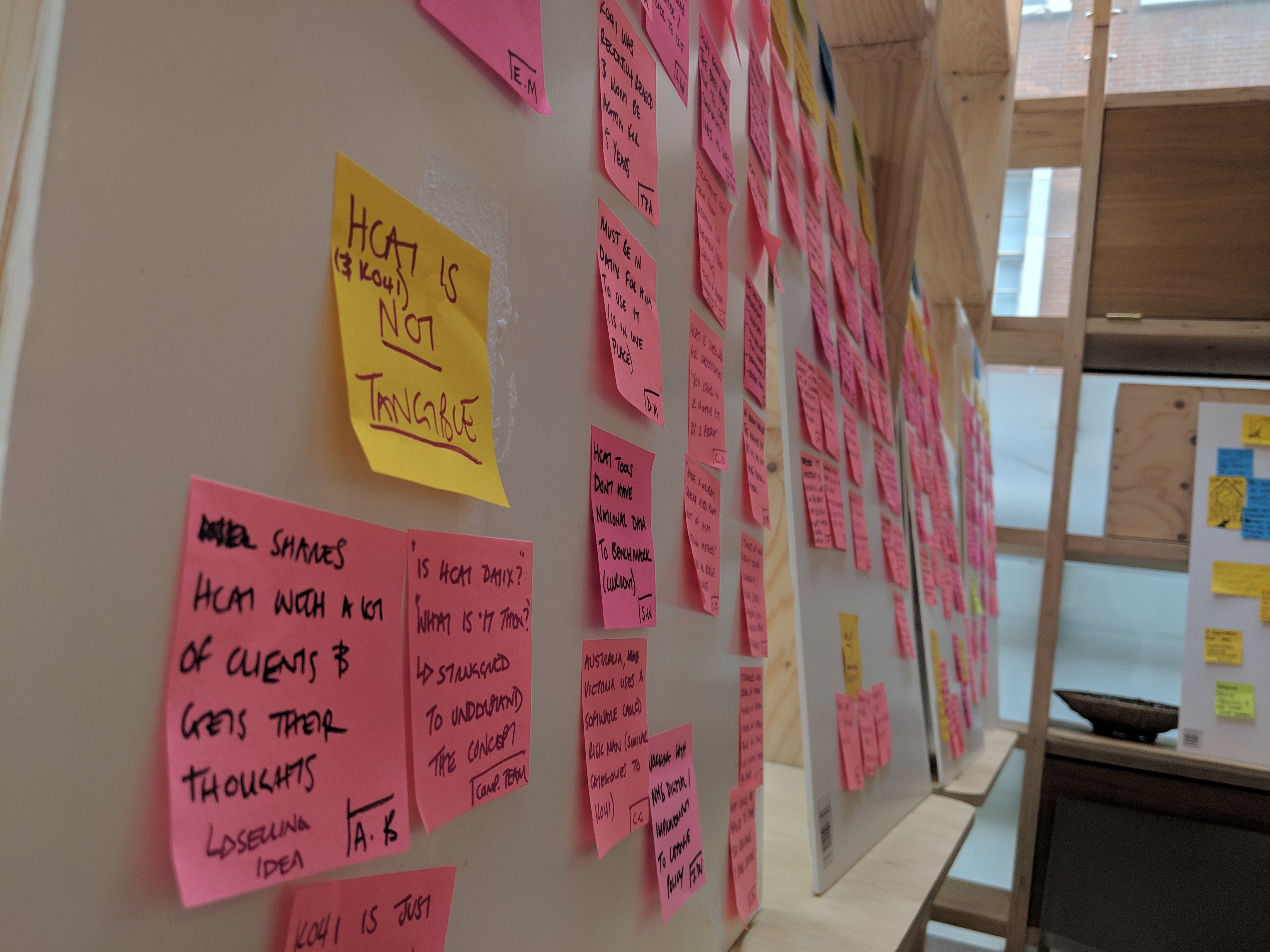
People’s unstructured feedback is difficult to navigate and laborious to extract meaningful insights from, particularly since the NHS receives some 570 written complaints every single day. Arguably, though, this is part of what makes the feedback so valuable.
“The unstructured nature of feedback is what provides the complexity,” says Pip Batey, designer at our Helix Centre. “But this complexity is also the value. Written feedback, especially complaints, are a rich narrative of personal experiences across multiple touchpoints within the system; hospitals, GP surgeries, community services, etc.”
So how do healthcare professionals begin to make sense of this melting pot of data?
“One solution is to categorise or ‘code’ this data to make it structured, so that it can be analysed more efficiently and, in turn, fed back to hospital wards in a meaningful way that can prompt change,” says Jackie van Dael, PhD student at IGHI’s NIHR Imperial Patient Safety Translational Research Centre.
“This is exactly what the Healthcare Complaints Analysis Tool does. The issue is, it’s a well-kept secret among the complaints community. We want to drive greater engagement with this tool so that patients and families can have a greater impact on health systems, and we hope our new platform, Feedback First, will help towards that goal.”
A catalyst for change
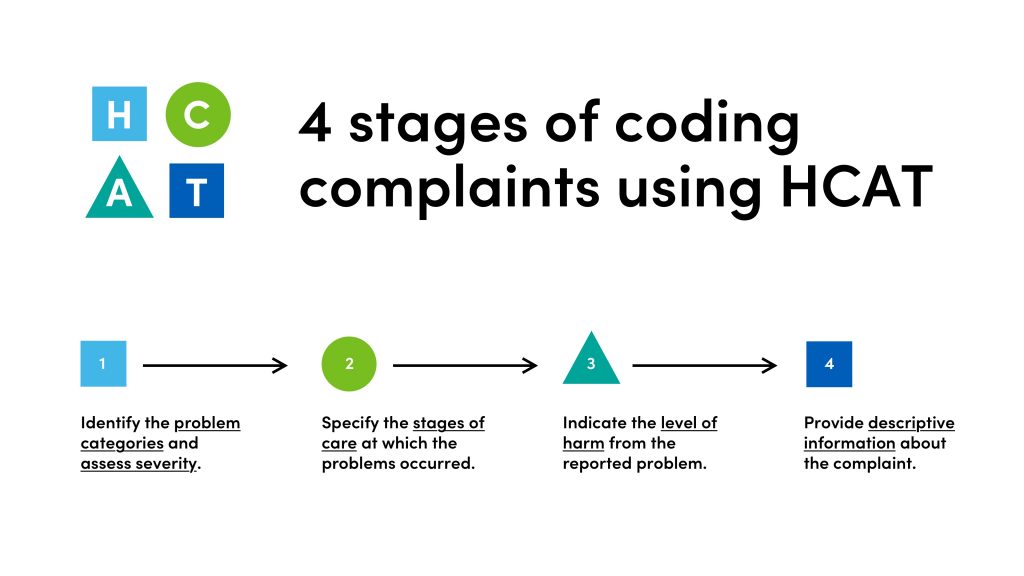
Developed at the London School of Economics, the Healthcare Complaints Analysis Tool (HCAT) is a coding method that allows organisations to standardise the way they analyse patient complaints, and thus turn them into an effective springboard for improvement. It’s a powerful tool with great potential, yet this has yet to be realised across much of the healthcare community.
Many professionals aren’t aware of HCAT, which is in part due to the fragmented nature of the complaints community.
How patient complaints are coded using HCAT
Professionals therefore have little opportunity to come together to share best practices, meaning few people know what works well and what doesn’t. Added to this is the fact that patient experience data exists in siloes across the NHS, taking many different forms such as complaints, PALS, social media comments, the Friends and Family Test, among others.
Cognisant of these issues, Jackie’s and Pip’s teams came together to find a solution that could help leverage HCAT and increase its potential as a driver of quality improvement.
The researchers interviewed and shadowed a range of people, from HCAT users to patient complaints teams, and coalesced all of this information to identify emerging themes and pain points.
“We then ran a number of workshops with different users and stakeholders – clinicians, members of complaints teams, patients and the public – to try to figure out people’s priorities and needs,” says Pip.
“We started off just looking at patient complaints, but then we realised these are part of a much wider world of patient feedback.”
One major finding, Jackie says, was that staff didn’t feel empowered to give feedback to their colleagues because there was a lack of consistency and clear policies on doing so.
“This work highlighted the need for a common language that can align the feedback process and profession, and a way to highlight existing evidence on best practices to give them credibility,” she adds. “This will, in turn, provide patients and families reassurance that their concerns are listened to, and learned from.”
A spotlight on patient complaints
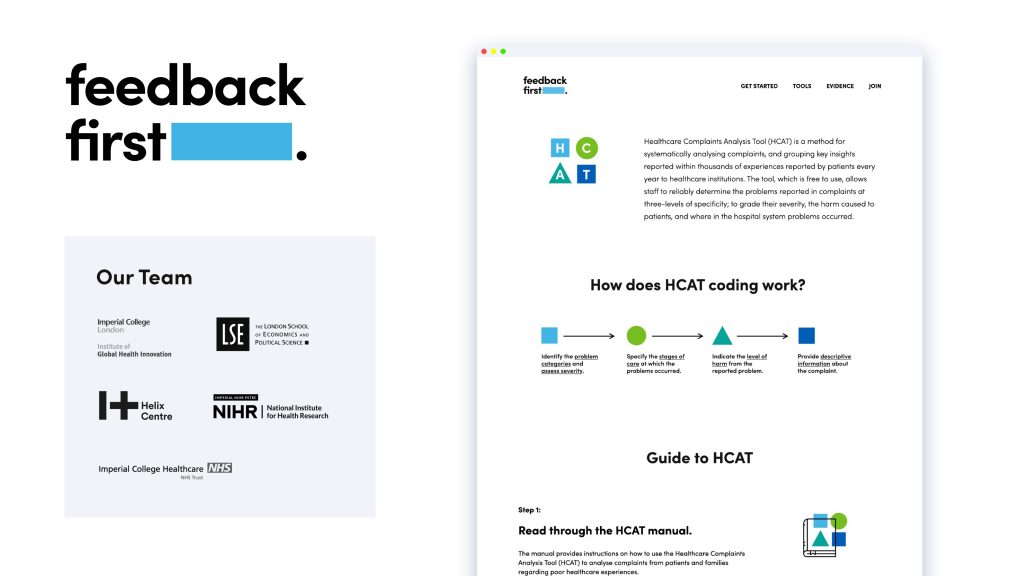
The team’s solution is simple. They’ve created a web-based platform for the feedback community – a toolbox for Trusts, researchers, and patient experience organisations to unite, share and learn. The idea is that this website, Feedback First, is a one-stop-shop for users to discover best practice tools, like HCAT; explore evidence that demonstrates the value of these tools, and connect with others who are seeking to make the most of patient feedback.
“By including a community section on the website, we hope to encourage people to take ownership of feedback, recognising that it’s everyone’s responsibility,” Pip says. “We’re also aiming to be a collaborative hub so that partners can join and bring in their analytical tools, enabling people to make sense of lots of different types of feedback data.”
No longer is the task of crunching thousands of comments seemingly impossible. But the end goal goes further than analysis. Ultimately, the team wants to use this data to trigger positive change in hospitals.
“In addition to traditional case-by-case complaint resolution, we want to help Trusts to systematically monitor trends in complaints data so that they can identify, for example, recurring or high severity complaints across the board,” Jackie says. “A tool like HCAT can help hospitals to visualise patient complaints data they get from using these tools. We call this ‘spotlight’ analysis.”
A snapshot of the Feedback First website
Scan, zoom, dissect
Spotlight analysis allows researchers to scan the high-level trends to spot areas that should be probed in finer detail. By performing further in-depth analyses of patients’ journeys through care, teams can then pick out lessons that Trusts can learn from and act on to prevent similar situations from happening in the future.
“It’s an antidote to the often fragmented and clinically-focused quality and safety data that is used in healthcare,” says Jackie, “which can be somewhat limited in providing a comprehensive picture of incidents or negligence.”
Our researchers hope these tools and techniques can enable Trusts to tangibly show how they’re responding to patients’ voices, and track the impact that resulting changes are having. It’s about listening, learning and improving.
It’s still early days for Feedback First, but the team hopes that growing this community is one important step towards safer, better quality healthcare.
If you’re interested in partnering with Feedback First, please contact Jackie (j.van-dael18@imperial.ac.uk) or Pip (pip@helixcentre.com) to find out more about this opportunity.
Taking medicines is the most common way that we attempt to stave off or treat illness. Every day people all across the world use medicines to help improve their health and wellbeing. They’ve transformed the treatment and outlook for many diseases, helping people live longer and healthier lives. Yet medicines are also a major risk to patients’ safety. And this risk is not only a result of drugs’ side effects.
Mistakes in the treatment process can also lead to patient harm. Errors can happen at any stage of the pathway; when professionals prescribe, dispense and administer drugs. In England alone, it’s estimated that over 230 million such errors occur every year, causing hundreds of deaths and contributing to thousands more. And the figure worldwide is just as grim. Medication errors cost countries across the world $42 billion annually.
That’s why our researchers want to make medicines safer, and their latest research highlights a remarkably simple solution that could help towards this goal. Published in BMJ Quality and Safety, they’ve found that basic tools for patients to record their own medication information – like paper ‘passports’ and mobile apps – could help to lower some of the risks associated with medicines. Encouraging more people to use these simple interventions could lead to greater patient empowerment, the researchers say, and enhance the safety of their care.
Obstacles to ownership
When patients move from one care setting to another – for example transitioning from hospital to the community – mistakes can happen in their care. Often this is because the systems aren’t well joined-up, meaning that patients’ information isn’t transferred properly. When this happens, patients are sometimes relied on to recount their own medical details to fill in the gaps. Not only is this frustrating for patients, but it leaves room for error if they forget certain bits of information, such as details of the medications they’re taking.
Supporting patients or their carers to be more involved in their medication could potentially help the flow of information during this process, and therefore lower some of the risks associated with transitions of care. One approach to facilitate such patient empowerment is the use of tools that our researchers refer to as ‘PHIMed’, or patient-held information about medicines. These could be a written record of their current and past treatment history, or digital apps that store the same information.
Previous research has identified some of the barriers to using PHIMed, but our researchers wanted to know more about them. They also wanted to better understand how these tools could help reduce the risks of medication errors happening.
Professor Bryony Dean Franklin and Dr Sara Garfield led the research. They interviewed two groups of patients and carers, and 16 healthcare professionals, including doctors, nurses, pharmacists, dentists and opticians. They next interviewed 60 people who use PHIMed. The research team then combined this information with existing literature to come up with a list of the most desired features of these tools, and tested several commonly used ones – both digital and paper – with a group of people to see if they matched up to people’s needs.
Finding the right match
The researchers found that many patients and carers don’t use PHIMed. People often didn’t realise the need for these tools, because they believed that accurate and up-to-date information about their medicines would be automatically available. “We were surprised that people thought healthcare information systems were all connected,” said Prof Franklin, who leads IGHI’s medication safety research. “Participants quickly considered carrying information about medicines when they found out they weren’t.”
But people who did already use PHIMed found these tools to be very helpful – as did healthcare professionals. The researchers found that patients and carers used a wide range of both paper and digital tools – from medicine passports and medical alert cards, to making notes on smartphones or using health apps. Although people generally used paper tools, the work highlighted how different people have different needs and preferences and that no single tool matched everyone’s wish list of key features.
“We found different types of PHIMed are likely to be best for different people – there’s no ‘one-size-fits-all’ solution that we should be recommending,” said Dr Sara Garfield. “Instead, it’s more important that people find a solution that works for them.”
Joining the dots
Importantly, the work also identified how these tools can help make medicines safer. Users and professionals reported that PHIMed helped ensure a complete and accurate list of medicines. By filling in gaps in patchy records, they smoothed the process of information transfer between care settings. They also seemed to empower patients to take ownership of their health, enabled better monitoring of conditions over time, and allowed patients and professionals to track whether medicines were working or not.
On top of this, one scenario where PHIMed may be particularly important is in emergency situations. In these cases patients may be unable to communicate with professionals and their carer may not be present to do so.
A step towards safer medicine use
As such a simple way to enable better communication about medicines, and therefore facilitate their safe use, the researchers hope that research like this will help to promote the benefits of PHIMed and encourage their uptake.
“We need to raise awareness of the purpose and value of carrying PHIMed among patients, carers and healthcare professionals alike,” said Prof Franklin. “Our findings suggest that many more people may be willing to carry it if they knew how helpful it could be.”
But such endeavours should avoid a bias towards one type of tool over another. Instead, they should empower patients and carers to find a method that works for them.
“Everyone is different, so we need to help patients to find the PHIMed tool that best suits their needs,” added Dr Garfield.
“PHIMed isn’t a panacea for medication errors. But it is one small step that we hope more people will take to enhance the safety of their healthcare.”
By Gianluca Fontana and Saira Ghafur, Centre for Health Policy
Our National Health Service owns some of the most comprehensive patient data sets across the globe. This makes these data a very valuable asset – not just as a springboard for improving health and care through learning from the data, but also in terms of the potential for financial return. It is critical that if the NHS shares this data with companies, in an appropriate and secure way, it also receives a fair share of this financial return.
These are arguments we make in a new article published in Lancet Digital Health. We also highlight the need for a wide and transparent debate on this topic, alongside making some key recommendations for policy and practice change in this area. By taking these critical actions, we believe that we all stand to benefit – both as patients and taxpayers.
The value of NHS data
Healthcare data is extremely valuable. Through increasing our understanding of health and how healthcare systems are working, it has the potential to make care more effective and efficient. Thus, improving patient outcomes and financial sustainability. In other words, it can help providers and health systems, like the NHS in the UK, get better at what they do.
It can also enable the discovery of new drugs or the development of new technologies, including digital health applications and artificial intelligence algorithms. Accessing healthcare data is therefore a priority for businesses and research institutions, which traditionally drive this type of innovation. In doing so, they certainly can help develop a better future for our healthcare systems.
However, giving access to sensitive data, even in anonymised form, to private organisations is something that the public has often expressed concerns about or rejected altogether. It is therefore critical that if the data is shared, it is done with the awareness and support of the public. And, according to secure and well-defined processes. Shortcuts should be avoided. The public should also be properly consulted and listened to, not nudged towards what policy wonks like us, even if well-meaning, think is right.
The issue of how to share the financial value generated from healthcare data merits a lot more attention and discussion than what has been the case so far. If NHS data leads to successful products or innovations, should the NHS receive something in return? We believe the answer is yes.
Ways to ensure a fair share
Our recent article in the Lancet Digital Health is an attempt to start a more vibrant and wider debate on this topic. We believe this should involve the public, healthcare practitioners, policy-makers, academics and colleagues from the private sector.
In the article, we suggest the need for an updated policy and decision-making framework to ensure that the NHS realises fair financial value from its data. We strongly recommend that NHS organisations consider a wide range of mechanisms to capture some of the value, including:
Getting free or discounted access to products developed from the data
Receiving a one-off payment in exchange for data access or a series of one-off payments based on regulatory and commercial milestones
Receiving a royalty payment or share of the revenue from the products that are developed using the data (including by leveraging shared ownership of intellectual property generated in connection with the partner’s data mining)
Receiving a share of the profits of the company commercialising the data
Receiving a share of the equity in the company commercialising the data
Receiving a so-called ‘golden share’, which in specific predetermined circumstances can out-vote all other shares in the company commercialising the data
The right approach will vary from case to case, but it is important to consider the full range of options.
It is critical that this issue is discussed more widely and that an approach supported by the public is identified and implemented. As shown by recent press coverage and by the debate leading up to the last UK general election, less-than-transparent or rushed attempts to take action in this area are likely to generate significant resistance, and to negatively impact trust in the NHS and the progress towards a better, data-supported future in healthcare.
Gianluca Fontana is the Director of Operations at IGHI’s Centre for Health Policy. Dr Saira Ghafur is the Centre’s Lead for Digital Health.
Lighting up the Queen’s Tower in honour of World Patient Safety Day was just one of our many proud moments this year.
As the year draws to a close, we look back at some of IGHI’s best moments over the past 12 months. From launching new trials to test out promising health innovations, to partnering for better mental health, our Institute has achieved many things we’re proud of.
Find out how our progress is leading us towards our ambition of transforming health and care for all. (more…)
Xbox tech could soon offer a helping hand in operating theatres
Many will be wishing to discover an Xbox-shaped gift glittering under the Christmas tree this year. Aside from the seemingly endless hours of entertainment, joy, frustration and competition that these consoles offer, Xbox technology – and other similar gadgets – is finding uses outside of the gaming world, and in the healthcare research sphere. (more…)