Fourth and final week at the Royal Hospital for Neuro-disability
My final week at the Royal Hospital for Neuro-disability (RHN) has revealed that inevitably I’m not the only person examining the possibilities for improved seating design. From car seats to desk chairs to wheelchairs, the message is always the same; using new technologies future seats can and need to be better designed around the human body. There’s an asterisk on the end of that phrase though: the sheer amount of variation doesn’t make this an easy task. To this end a great deal of time this week has been spent reading through academic papers examining different aspects or users of all sorts of chairs, and obtaining the many papers referenced in each. The result is that I have more papers to go through than I started with earlier this week, and I run the risk of adding to an exponentially increasing stockpile!
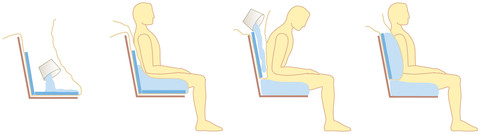
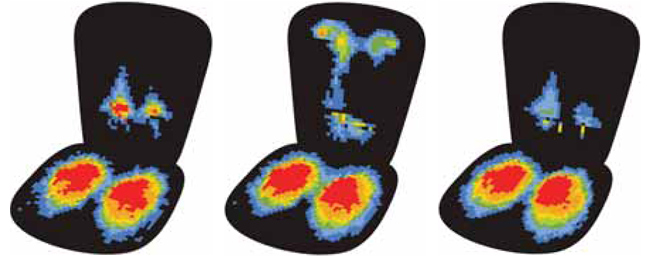
To summarise my findings so far; the prevailing opinion is that spreading the person’s weight as evenly as possible over the seat contact area is the best way to prevent long-term seating injury for the reasons discussed in my Week 2 post. On the other hand a few papers suggest that reducing the pressure over certain weaker parts of the rear and maximising the pressure around the area underneath the strong pelvis bone is the best way forward. Depending on which theory was supported, various researchers have developed methods and devices to shape the seat to best fit the patient. One example used an array of sliding upright rods fitted with pressure and location sensors on which the patient sat to create a set of points in 3D space that represent the contours of the chair. A linked computer would then examine the measured pressure at each rod location and slide the rods up or down while the patient was still seated to achieve a better pressure distribution. The adjusted 3D point set would then be used by automated tools to manufacture the seat. The biggest problem with many of these solutions is the cost and practicability of implementing them alongside recommendations by trained therapists, who are conventionally responsible for gauging a disabled patient’s mobility and seating needs.
This project was always intended to be a first step in investigating possible solutions to future wheelchair designs for severely disabled patients. After conducting research towards this aim, focussing in particular on improving the seat design, I can confirm that there is a great deal more juice in this project yet. The hospital has therefore agreed that I continue this project, with the aim of submitting a report on the progress of the project and possible design solutions at the end of the summer. Some prototyping along the way is a strong possibility!
I have definitely enjoyed the last 4 weeks, meeting new people at the hospital and engaging in fascinating discussions with them. These have opened not only my eyes to the reality of caring for disabled patients, but have also caused the staff to ask themselves new questions and challenge the conventional ways of designing wheelchairs and wheelchair seats. As well as reading a great deal into the research topics, I have through trial and error experimented with new ways to organise and structure my research that will no doubt help in the years to come.
Best of luck to all those also completing their Charity Insights placements this summer. If you’re reading this while considering completing a Charity Insights placement in the future, believe me it’s well worth it!